You might also like
- Statistical Methods for Evaluating Safety in Medical Product DevelopmentFrom EverandStatistical Methods for Evaluating Safety in Medical Product DevelopmentA. Lawrence GouldNo ratings yet
- Eli Lilly Biotech Pilot Plant, Indianapolis, United States of AmericaDocument5 pagesEli Lilly Biotech Pilot Plant, Indianapolis, United States of AmericaShyam Sunder BudhwarNo ratings yet
- Biological Evaluation of Medical Devices / Biosafety: Applicable ProductsDocument5 pagesBiological Evaluation of Medical Devices / Biosafety: Applicable ProductsAnonymous iqoU1mtNo ratings yet
- Iec62304 3Document5 pagesIec62304 3Abdul RahmanNo ratings yet
- ISO 18113-1 2022 Ed.2 - Id.79866 Publication PDF (En)Document60 pagesISO 18113-1 2022 Ed.2 - Id.79866 Publication PDF (En)Qualidade FrilaboNo ratings yet
- Cleaning and Sterilization GuideDocument48 pagesCleaning and Sterilization GuideFrankArenasNo ratings yet
- Rockwell Software Product CatalogDocument36 pagesRockwell Software Product CatalogAdhemar RodoNo ratings yet
- Lecture7 Introduction To Medical Devices ManagementDocument7 pagesLecture7 Introduction To Medical Devices ManagementRula BastoniNo ratings yet
- ZFP Op Man - EN PDFDocument142 pagesZFP Op Man - EN PDFMohamed Abd El-Fattah GalalNo ratings yet
- Regulatory Samvad Feb 2020Document19 pagesRegulatory Samvad Feb 2020vibhu yadavNo ratings yet
- Bioinformatics CompaniesDocument18 pagesBioinformatics Companiesmy.dear.sirNo ratings yet
- Principles of Software EngineeringDocument2 pagesPrinciples of Software EngineeringKr UthayanNo ratings yet
- Lecture4 Introduction To Medical Devices ManagementDocument9 pagesLecture4 Introduction To Medical Devices ManagementRula BastoniNo ratings yet
- Pacs (Picture Archiving and Communication Systems) & Vna (Vendor Neutral Archives)Document18 pagesPacs (Picture Archiving and Communication Systems) & Vna (Vendor Neutral Archives)LawrenceNo ratings yet
- Auditing Operating Systems Networks: Security Part 1: andDocument24 pagesAuditing Operating Systems Networks: Security Part 1: andAmy RillorazaNo ratings yet
- Defect Tracking SystemDocument21 pagesDefect Tracking Systemmughees1050% (2)
- High Performance Medical Grade Resins PDFDocument11 pagesHigh Performance Medical Grade Resins PDFGeorge CobraNo ratings yet
- ART - 0608 - Improving Ops With EBRDocument4 pagesART - 0608 - Improving Ops With EBRkumar_chemicalNo ratings yet
- Recent Trends in Sterile InspectionsDocument40 pagesRecent Trends in Sterile InspectionsSilke IgemannNo ratings yet
- Data Integrity & SecurityDocument3 pagesData Integrity & SecurityReshma WawhalNo ratings yet
- McKesson Letter of FDA's Proposed Medical Device Data Systems RuleDocument5 pagesMcKesson Letter of FDA's Proposed Medical Device Data Systems RulehuffpostfundNo ratings yet
- Detailed Design Specification TemplateDocument8 pagesDetailed Design Specification Templatemaddy_cooldude6763No ratings yet
- IntegrityDocument25 pagesIntegrityChhatrashal Singh RathoreNo ratings yet
- Glucometer SRSDocument15 pagesGlucometer SRSYisha XiaNo ratings yet
- Competitive Analysis of Market Leaders in Data ModelingDocument24 pagesCompetitive Analysis of Market Leaders in Data ModelingXavier Martinez Ruiz100% (2)
- SBSI CoagulationDocument3 pagesSBSI Coagulationjay primaNo ratings yet
- Global Medical Device Nomenclature: Mark Wasmuth Secretary General GMDN AgencyDocument23 pagesGlobal Medical Device Nomenclature: Mark Wasmuth Secretary General GMDN AgencyluNo ratings yet
- Seven Principles of Software TestingDocument3 pagesSeven Principles of Software TestingpedromoritzNo ratings yet
- Dell EMC Validates Your Virtualized Genetec Video Management System Before It Reaches Your HandsDocument11 pagesDell EMC Validates Your Virtualized Genetec Video Management System Before It Reaches Your HandsPrincipled TechnologiesNo ratings yet
- GMP 2023 - Sessions PresentationsDocument289 pagesGMP 2023 - Sessions PresentationsKamanashish Chowdhury100% (1)
- Automated Packaging Systems Autolabel Pi-4000 In-Line, Programmable, Thermal Transfer PrinterDocument2 pagesAutomated Packaging Systems Autolabel Pi-4000 In-Line, Programmable, Thermal Transfer PrinterEdgar HoowerNo ratings yet
- SharePoint 2013 Qualif. Pack List-1Document2 pagesSharePoint 2013 Qualif. Pack List-1akbarmulangathNo ratings yet
- Software Quality EnginneringDocument26 pagesSoftware Quality EnginneringVinay PrakashNo ratings yet
- Research Paper Artificial Intelligence in Medical JEEV AI-IJRASETDocument8 pagesResearch Paper Artificial Intelligence in Medical JEEV AI-IJRASETIJRASETPublicationsNo ratings yet
- 03 System TestingDocument17 pages03 System TestingramNo ratings yet
- Data Validation, Processing, and Reporting Data ValidationDocument8 pagesData Validation, Processing, and Reporting Data ValidationNaga Ajay Kumar DintakurthiNo ratings yet
- Aplicabilidad 21CFR11Document6 pagesAplicabilidad 21CFR11Aydee RojasNo ratings yet
- Symbient PRD TemplateDocument5 pagesSymbient PRD TemplateBikash Chandra SahooNo ratings yet
- Test Design Specification TemplateDocument4 pagesTest Design Specification TemplateRifQi TaqiyuddinNo ratings yet
- SDLCDocument22 pagesSDLCRishabh AroraNo ratings yet
- What Is JIRA?: Issue: Every Task, Bug, Enhancement Request BasicallyDocument1 pageWhat Is JIRA?: Issue: Every Task, Bug, Enhancement Request Basicallylilithknowsitall6393No ratings yet
- Oven ManualDocument28 pagesOven ManualromwellNo ratings yet
- Backup and Recovery Best Practices For Leadership and PlanningDocument5 pagesBackup and Recovery Best Practices For Leadership and PlanningVijay Jangetti SanjeeviNo ratings yet
- FDA Design Considerations For Devices Intended For Home UseDocument27 pagesFDA Design Considerations For Devices Intended For Home Use0SpYkeNo ratings yet
- Manufacturing Execution System (MES) : ServiceDocument48 pagesManufacturing Execution System (MES) : ServiceNhat Tan MaiNo ratings yet
- Smart Lab E BookDocument24 pagesSmart Lab E BookNaveed MubarikNo ratings yet
- Strategic Management and Project Management: PurposeDocument10 pagesStrategic Management and Project Management: PurposesurapolNo ratings yet
- Road Map To Design Successful Software - Ictms (Integrated Clinical Trial Management System)Document8 pagesRoad Map To Design Successful Software - Ictms (Integrated Clinical Trial Management System)SanjayPravinbhaiVarmaNo ratings yet
- Requirement Engineering SummaryDocument14 pagesRequirement Engineering SummaryBob ChanNo ratings yet
- Seilevel Agile Requirements Document TemplateDocument10 pagesSeilevel Agile Requirements Document TemplateSanoufar ANo ratings yet
- GMP Simatic Pcs7-V90 en En-UsDocument184 pagesGMP Simatic Pcs7-V90 en En-UshuykhiemNo ratings yet
- Broch Biostat-STR-Flexsafe SBI1509-e NeuDocument24 pagesBroch Biostat-STR-Flexsafe SBI1509-e NeuBrian VasquezNo ratings yet
- FDA Pre Submission Cover LetterDocument5 pagesFDA Pre Submission Cover Letteregdxrzadf100% (2)
- Medical Product DevelopmentDocument64 pagesMedical Product DevelopmentIhsanNo ratings yet
- CDRH201461 HomeUseDesign FinalGuidanceDocument27 pagesCDRH201461 HomeUseDesign FinalGuidancerehmanabbasiNo ratings yet
- Unique Device IdentificationDocument15 pagesUnique Device IdentificationSureshNo ratings yet
- AG3110 - Vue PACS and Vue Archive 12.2 Administration GuideDocument177 pagesAG3110 - Vue PACS and Vue Archive 12.2 Administration GuideAndreia Yamamoto MorassutiNo ratings yet
- Sferd Handbook Flexible Endoscopes Cleaning Disinfection - en PDFDocument106 pagesSferd Handbook Flexible Endoscopes Cleaning Disinfection - en PDFmochkurniawanNo ratings yet
- Software ArchitectureDocument30 pagesSoftware ArchitectureMukesh RegmiNo ratings yet
- Labelling Nutrition-Vitamins Minerals-Guidance Tolerances Summary Table 012013 enDocument1 pageLabelling Nutrition-Vitamins Minerals-Guidance Tolerances Summary Table 012013 enDaniela CirnatuNo ratings yet
- 202103011101-Ghid de Prevenire Iaam 2021Document52 pages202103011101-Ghid de Prevenire Iaam 2021Daniela CirnatuNo ratings yet
- Notification File Food Supplement / Fortified Food: OmpanyDocument4 pagesNotification File Food Supplement / Fortified Food: OmpanyDaniela CirnatuNo ratings yet
- Disinfection and SterilizationDocument23 pagesDisinfection and SterilizationDaniela Cirnatu100% (1)
- Mayo Clinic Proceedings: Vitamin D Supplementation During The COVID-19 PandemicDocument2 pagesMayo Clinic Proceedings: Vitamin D Supplementation During The COVID-19 PandemicDaniela CirnatuNo ratings yet
- Patient Identity NicknameDocument2 pagesPatient Identity NicknameDaniela CirnatuNo ratings yet
- 11.5 ArsenicDocument18 pages11.5 ArsenicDaniela CirnatuNo ratings yet
- Hepatorenal and Genotoxic Effects of Genetically Modified Quail Meat in A 90-Day Dietary Toxicity Study in MiceDocument7 pagesHepatorenal and Genotoxic Effects of Genetically Modified Quail Meat in A 90-Day Dietary Toxicity Study in MiceDaniela CirnatuNo ratings yet
- CXS - 197e Norma Codex AVOCADO Draft EnglishDocument6 pagesCXS - 197e Norma Codex AVOCADO Draft EnglishDaniela CirnatuNo ratings yet
- Chemistry Investigatory ProjectDocument19 pagesChemistry Investigatory ProjectDivya Vatsa50% (4)
- Study On Detergent PowderDocument12 pagesStudy On Detergent PowderRamesh Choudhary100% (2)
- Spectracron 110 FD Alkyd Enamel PDFDocument2 pagesSpectracron 110 FD Alkyd Enamel PDFSatish Vishnubhotla0% (1)
- Analysis of Cement by Banana FiberDocument48 pagesAnalysis of Cement by Banana FiberKyaw KhineNo ratings yet
- Chapter 9 The Endocrine SystemDocument1 pageChapter 9 The Endocrine SystemacNo ratings yet
- Chemistry Investigatory Project 2017-18Document29 pagesChemistry Investigatory Project 2017-18Ashok KumarNo ratings yet
- Realistic Well Planning With Dynamic Well Control ModellingDocument7 pagesRealistic Well Planning With Dynamic Well Control ModellingAoun MuhammadNo ratings yet
- 30 Sewage Treatment PlanDocument63 pages30 Sewage Treatment PlanYuri Duri100% (1)
- Final Examination: Your Answer On The Space Provided For. (40 Points)Document5 pagesFinal Examination: Your Answer On The Space Provided For. (40 Points)Wichel AnnNo ratings yet
- Carbon NanotubesDocument15 pagesCarbon NanotubesLaraib HabibNo ratings yet
- Universitas Ahmad Dahlan - JellyDocument15 pagesUniversitas Ahmad Dahlan - JellyMaqfirotul LailyNo ratings yet
- Trepanning Positioning Welding ManualDocument14 pagesTrepanning Positioning Welding ManualGovindan PerumalNo ratings yet
- S Start of Lesson E End of Lesson Grading 1-5: Learning Outcomes Progress ArrowDocument30 pagesS Start of Lesson E End of Lesson Grading 1-5: Learning Outcomes Progress ArrowYu Seung KimNo ratings yet
- Mil PRF 9954DDocument8 pagesMil PRF 9954DjhscribdaccNo ratings yet
- Single Phase Heat Transfer and Pressure Drop Characteristics of Micro-Fin TubesDocument2 pagesSingle Phase Heat Transfer and Pressure Drop Characteristics of Micro-Fin TubesGerehNo ratings yet
- 11 - Isomerism in TMCDocument18 pages11 - Isomerism in TMCMohit KambojNo ratings yet
- Eucomex - Eucomex - EnglishDocument2 pagesEucomex - Eucomex - EnglishNelson IbarraNo ratings yet
- Simulation of Reactive Distillation ColumnDocument6 pagesSimulation of Reactive Distillation ColumnthanhndbNo ratings yet
- Special Issue Honoring Don Mackay: Oil Spill Impact Modeling: Development and ValidationDocument16 pagesSpecial Issue Honoring Don Mackay: Oil Spill Impact Modeling: Development and Validationbrice mouadjeNo ratings yet
- 4 Elements, Mixtures and Compounds: WorksheetDocument3 pages4 Elements, Mixtures and Compounds: WorksheetMfanafuthiNo ratings yet
- Toxicity of Common Laboratory Chemicals To Human Red Blood Cells Laboratory ActivityDocument4 pagesToxicity of Common Laboratory Chemicals To Human Red Blood Cells Laboratory ActivityKuven Malig-onNo ratings yet
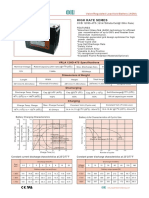
- High Rate Series: CCB 12HD-475Document1 pageHigh Rate Series: CCB 12HD-475orunmila123No ratings yet
- Rusting WorksheetDocument2 pagesRusting WorksheetSelwah Hj AkipNo ratings yet
- Magnetic Terms and UnitsDocument3 pagesMagnetic Terms and UnitsDeepak Choudhary DCNo ratings yet
- Advanced Inorganic Chemistry (CHM4301) : Alkenes and AlkynesDocument19 pagesAdvanced Inorganic Chemistry (CHM4301) : Alkenes and AlkynesAnonymous lClX1bNo ratings yet
- Jotun Penguard Express CF TDSDocument5 pagesJotun Penguard Express CF TDSnihad_mNo ratings yet
- Name: Grade & Section: Teacher: Score: General Direction: This Is A 50-Item Test, Read Each Direction Written in Every Type of Test, Answer ThisDocument4 pagesName: Grade & Section: Teacher: Score: General Direction: This Is A 50-Item Test, Read Each Direction Written in Every Type of Test, Answer ThisMara LabanderoNo ratings yet
- Hot Tap ProcedureDocument6 pagesHot Tap ProcedureNatarajan MurugesanNo ratings yet
- 2002Document38 pages2002B GirishNo ratings yet
- Pulp Mill Odor ControlDocument6 pagesPulp Mill Odor Controlalakazum28No ratings yet