You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Nematode Biology, Physiology & Ecology - Conversion GateDocument42 pagesNematode Biology, Physiology & Ecology - Conversion GatePra YoudhaNo ratings yet
- Comparing Animal and Plant Cell Structures and FunctionsDocument30 pagesComparing Animal and Plant Cell Structures and FunctionsNetty BontuyanNo ratings yet
- Clinic VisitDocument5 pagesClinic VisitEka YunusNo ratings yet
- Potato Poisoning: Understanding Solanine ToxicityDocument13 pagesPotato Poisoning: Understanding Solanine ToxicityDaz Jones100% (2)
- Dental Management in Hematologic DisordersDocument31 pagesDental Management in Hematologic DisordersdmdsahNo ratings yet
- 3.0 Cytology-CELL CYCLE UphmoDocument43 pages3.0 Cytology-CELL CYCLE UphmoPatrick DingcoNo ratings yet
- CNS Stimulants 2023Document10 pagesCNS Stimulants 2023ManWol JangNo ratings yet
- Cooperative Activity 3-1 Through 3-3Document3 pagesCooperative Activity 3-1 Through 3-3Thalia Sanders100% (2)
- Identifying Amino AcidsDocument8 pagesIdentifying Amino AcidsWahyuniAntariNo ratings yet
- Sleep Disorders in Children and Adolescents: Understanding Causes and Treatment OptionsDocument50 pagesSleep Disorders in Children and Adolescents: Understanding Causes and Treatment OptionsCitra Sukri Sugesti100% (1)
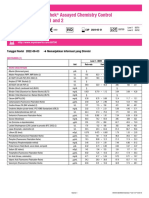
- Lyphochek Assayed Chemistry Control Levels 1 and 2: Tanggal Revisi 2022-06-03 Menunjukkan Informasi Yang DirevisiDocument2 pagesLyphochek Assayed Chemistry Control Levels 1 and 2: Tanggal Revisi 2022-06-03 Menunjukkan Informasi Yang DirevisiFahmiNo ratings yet
- MS Case PresDocument33 pagesMS Case PresShaine_Thompso_6877No ratings yet
- Patient Scenario, Chapter 19, Nutritional Needs of A NewbornDocument3 pagesPatient Scenario, Chapter 19, Nutritional Needs of A NewbornNobiliary ortizNo ratings yet
- A Monster Calls - ExtractDocument2 pagesA Monster Calls - ExtractJo PatrickNo ratings yet
- (VCE Biology) 2007 Chemology Unit 1 Exam and SolutionsDocument28 pages(VCE Biology) 2007 Chemology Unit 1 Exam and SolutionsJustine LyNo ratings yet
- Stages of SleepDocument2 pagesStages of SleepCamilia Hilmy FaidahNo ratings yet
- Neuropsychoanalysis - The Concious ID Solms PDFDocument16 pagesNeuropsychoanalysis - The Concious ID Solms PDFAndrei PredaNo ratings yet
- MalariaDocument3 pagesMalariasuciNo ratings yet
- Photosynthesis WorksheetDocument3 pagesPhotosynthesis WorksheetByambazaya E100% (2)
- Effects of Ureteral Obstruction on Renal Hemodynamics and FunctionDocument19 pagesEffects of Ureteral Obstruction on Renal Hemodynamics and FunctionBayu HernawanNo ratings yet
- Bipap A30 Specification / Part NumbersDocument2 pagesBipap A30 Specification / Part NumbersDejan ŽujovićNo ratings yet
- Elec Eng 3Bb3:: Cellular BioelectricityDocument15 pagesElec Eng 3Bb3:: Cellular BioelectricityJens RydNo ratings yet
- Using Front-End Kinetics To Optimize Target-Controlled Drug InfusionsDocument9 pagesUsing Front-End Kinetics To Optimize Target-Controlled Drug InfusionsSilvyNo ratings yet
- Muscular TissuesDocument46 pagesMuscular TissuesDAVE CANALETANo ratings yet
- Latihan Organ Pernafasan Haiwan Animals Breathing OrgansDocument5 pagesLatihan Organ Pernafasan Haiwan Animals Breathing OrgansSangkaran KaranNo ratings yet
- Problems with Polyvagal TheoryDocument6 pagesProblems with Polyvagal TheoryCamilo IgnacioNo ratings yet
- DM Type IiDocument5 pagesDM Type IiKay Clarice G. TimosaNo ratings yet
- Answer Guide For O Level Biology (5090/3) - Paper 3 Practical Test June 2001Document3 pagesAnswer Guide For O Level Biology (5090/3) - Paper 3 Practical Test June 2001MSHNo ratings yet
- Botany II PDFDocument7 pagesBotany II PDFMuhammad AmirNo ratings yet
- Biochemistry I Lecture on Cellular Organization and Energy in Living Systems/TITLEDocument16 pagesBiochemistry I Lecture on Cellular Organization and Energy in Living Systems/TITLECiara CaldwellNo ratings yet