You might also like
- Module 2 Vocabulary Lists Clinical and Grammatical SuffixesDocument4 pagesModule 2 Vocabulary Lists Clinical and Grammatical SuffixesEdith KuaNo ratings yet
- EOSC 310 Questions (UBC 2016)Document5 pagesEOSC 310 Questions (UBC 2016)Edith KuaNo ratings yet
- Tutorial 4 QuestionDocument4 pagesTutorial 4 QuestionEdith KuaNo ratings yet
- Dr. Etazaz Econometrics Notes PDFDocument98 pagesDr. Etazaz Econometrics Notes PDFMuhammadYunasKhan100% (1)
- Watson Introduccion A La Econometria PDFDocument253 pagesWatson Introduccion A La Econometria PDF131270No ratings yet
- Econ 427 Assignment 4 Instrumental Variables ModelsDocument4 pagesEcon 427 Assignment 4 Instrumental Variables ModelsEdith KuaNo ratings yet
- Econometrics Question and AnswerDocument7 pagesEconometrics Question and AnswerEdith KuaNo ratings yet
- 2015 Midterm SolutionsDocument7 pages2015 Midterm SolutionsEdith Kua100% (1)
- 03.econ427 2016 SW6Document41 pages03.econ427 2016 SW6Edith KuaNo ratings yet
- 06.Econ427C 2016 SW10Document73 pages06.Econ427C 2016 SW10Edith KuaNo ratings yet
- Econ 491: Econometrics Stock and WatsonDocument63 pagesEcon 491: Econometrics Stock and WatsonEdith KuaNo ratings yet
- 06.Econ427C 2016 SW10Document73 pages06.Econ427C 2016 SW10Edith KuaNo ratings yet
- IV - Exchange Rate DeterminationDocument40 pagesIV - Exchange Rate DeterminationEdith KuaNo ratings yet
- Intermediate Macroeconomics 205Document9 pagesIntermediate Macroeconomics 205Edith KuaNo ratings yet
- ECON 345 Money and Banking Chapter 2 Functions Markets IntermediariesDocument20 pagesECON 345 Money and Banking Chapter 2 Functions Markets IntermediariesEdith KuaNo ratings yet
- 5a. Organizational Lab HPW KEYDocument8 pages5a. Organizational Lab HPW KEYEdith Kua100% (2)
- ECON 345 Money and Banking Chapter 1 OverviewDocument27 pagesECON 345 Money and Banking Chapter 1 OverviewEdith KuaNo ratings yet
- IV - Exchange Rate DeterminationDocument40 pagesIV - Exchange Rate DeterminationEdith KuaNo ratings yet
- Why The West? (Ferguson)Document13 pagesWhy The West? (Ferguson)Andrew SernatingerNo ratings yet
- MacroeconomicsDocument4 pagesMacroeconomicsEdith KuaNo ratings yet
- How central bank actions impact pricesDocument5 pagesHow central bank actions impact pricesTatiana Rotaru0% (1)
- Instructor'S Manual: International TradeDocument206 pagesInstructor'S Manual: International Tradebigeaz50% (4)
- Economic History: Global Interactions (1450 - 1750)Document26 pagesEconomic History: Global Interactions (1450 - 1750)Edith KuaNo ratings yet
- Equation List For Lecture 1 - 4 (Till Jan 17)Document1 pageEquation List For Lecture 1 - 4 (Till Jan 17)Edith KuaNo ratings yet
- Lazear Gibbs 2007Document157 pagesLazear Gibbs 2007Edith KuaNo ratings yet
- New Era, New Responsibilities: 174 Vital Speeches of The DayDocument6 pagesNew Era, New Responsibilities: 174 Vital Speeches of The DayEdith KuaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- International Ayurvedic Medical Journal: Case Report ISSN: 2320 5091 Impact Factor: 4.018Document4 pagesInternational Ayurvedic Medical Journal: Case Report ISSN: 2320 5091 Impact Factor: 4.018triplete123No ratings yet
- Relaxant Effect of Thymus VulgarisDocument4 pagesRelaxant Effect of Thymus VulgarisgangaNo ratings yet
- Juan Bertran Figueras, History of Homeopathy in Spain (Catalonia)Document12 pagesJuan Bertran Figueras, History of Homeopathy in Spain (Catalonia)Maria-Neus Lorenzo-Galés100% (2)
- Communicable Disease Surveillance in Animal PopulationDocument15 pagesCommunicable Disease Surveillance in Animal Populationsamwel danielNo ratings yet
- Impact of Philippines' 4Ps cash transfer programme on healthcare and educationDocument3 pagesImpact of Philippines' 4Ps cash transfer programme on healthcare and educationJustine Martin PrejillanaNo ratings yet
- Acrylic Partial Dentures More Satisfying Than Cast DenturesDocument4 pagesAcrylic Partial Dentures More Satisfying Than Cast DenturesAkikoz N SevenNo ratings yet
- STELLA Edited 4-1Document41 pagesSTELLA Edited 4-1Okwany JimmyNo ratings yet
- Post Mortem CareDocument2 pagesPost Mortem Carebea pegadNo ratings yet
- Safeguarding Policy Analysis of An NHS TrustDocument14 pagesSafeguarding Policy Analysis of An NHS Trustrose muabeNo ratings yet
- Ethical Issues in Nursing Research:: Deontological PerspectiveDocument11 pagesEthical Issues in Nursing Research:: Deontological PerspectiveJM JavienNo ratings yet
- Neuropsychopharmacology The Fifth Generation of Progress: 5th EditionDocument2,054 pagesNeuropsychopharmacology The Fifth Generation of Progress: 5th EditiondanilomarandolaNo ratings yet
- License Application (LIC1558941)Document2 pagesLicense Application (LIC1558941)souq alkanzNo ratings yet
- CSC Job Portal: Mgo San Leonardo, Nueva Ecija - Region IiiDocument1 pageCSC Job Portal: Mgo San Leonardo, Nueva Ecija - Region Iiirandiey john abelleraNo ratings yet
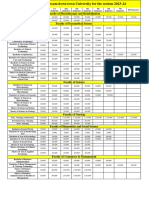
- Fees Structure Assam Down Town University For The Session 2023 2Document2 pagesFees Structure Assam Down Town University For The Session 2023 2Debashish SharmaNo ratings yet
- Maklumat Vaksinasi: Vaccination DetailsDocument2 pagesMaklumat Vaksinasi: Vaccination Detailsibrahim mohd rubaiNo ratings yet
- Amended Patient Classification Policy ManualDocument25 pagesAmended Patient Classification Policy ManualLaura Lopez GonzalezNo ratings yet
- Client Satisfaction and Quality of Health Care in Rural BangladeshDocument6 pagesClient Satisfaction and Quality of Health Care in Rural BangladeshMizanur RahmanNo ratings yet
- Chealthnet - OUR TEAMDocument2 pagesChealthnet - OUR TEAMshaikhbwcNo ratings yet
- Simple Triage and Rapid TreatmentDocument9 pagesSimple Triage and Rapid TreatmentGung IndrayanaNo ratings yet
- Legal Aspects of Perioperative NursingDocument9 pagesLegal Aspects of Perioperative NursingZerrie lei Hart100% (2)
- Memo No. 2022-59 - Submission of Updated PHIC and PRC License of Medical SpecialistsDocument8 pagesMemo No. 2022-59 - Submission of Updated PHIC and PRC License of Medical SpecialistsPaul Rizel LedesmaNo ratings yet
- Annual Report FY 2017-2018: Mobile Eye ClinicDocument18 pagesAnnual Report FY 2017-2018: Mobile Eye ClinicUMEC Young Professionals InitiativeNo ratings yet
- Suvarnaprashana Therapy in Children ConcDocument3 pagesSuvarnaprashana Therapy in Children ConcBhavana GangurdeNo ratings yet
- UK M P 004 v6.0 User-ManualDocument21 pagesUK M P 004 v6.0 User-ManualdrumerNo ratings yet
- Public Health Nurse PHN Final Exam Past Questions For WAHEBDocument3 pagesPublic Health Nurse PHN Final Exam Past Questions For WAHEBCharles Obaleagbon86% (7)
- Final Coaching Part and B - StudentDocument15 pagesFinal Coaching Part and B - StudentAshley Ann Flores100% (1)
- Speech Adult Case History - NLDocument4 pagesSpeech Adult Case History - NLHarshit AmbeshNo ratings yet
- Nutrition Career Guide - Definition, Objectives & AreasDocument6 pagesNutrition Career Guide - Definition, Objectives & Areastomas rNo ratings yet
- EBP Manual: A Guide to Evidence-Based PracticeDocument53 pagesEBP Manual: A Guide to Evidence-Based PracticesyamafiyahNo ratings yet
- Brgy. Talandang and Baganihan 2022 ConsolidatedDocument6 pagesBrgy. Talandang and Baganihan 2022 Consolidatedevelyn d. pepitoNo ratings yet