You might also like
- Intraplatelet Serotonin in Patients With Diabetes Mellitus and Peripheral Vascular DiseaseDocument6 pagesIntraplatelet Serotonin in Patients With Diabetes Mellitus and Peripheral Vascular DiseaseHyeon DaNo ratings yet
- Stratified Treatment of HypertensionDocument7 pagesStratified Treatment of HypertensionMohamad MuntahaNo ratings yet
- Hyperbilirubinemia: A Risk Factor For Infection in The Surgical Intensive Care UnitDocument14 pagesHyperbilirubinemia: A Risk Factor For Infection in The Surgical Intensive Care UnitChristian Karl B. LlanesNo ratings yet
- Parámetros Inflamatorios y Lipídicos en RDWDocument7 pagesParámetros Inflamatorios y Lipídicos en RDWJesus D. Hernandez GuitianNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderFrom EverandComplementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderNo ratings yet
- FluidDocument190 pagesFluidAndrias OzNo ratings yet
- HK 3Document6 pagesHK 3gekayuuNo ratings yet
- NAFLD and microalbuminuria in prediabetesDocument4 pagesNAFLD and microalbuminuria in prediabetesBinaNuraeniNo ratings yet
- A Comparison of The Pattern of Liver Involvement in Dengue Hemorrhagic Fever With Classic Dengue FeverDocument5 pagesA Comparison of The Pattern of Liver Involvement in Dengue Hemorrhagic Fever With Classic Dengue FeverMichelle Rayvi J. SumampouwNo ratings yet
- Assessment and Treatment of Hyperglycemia in Critically IllDocument6 pagesAssessment and Treatment of Hyperglycemia in Critically IllYousif ElmasryNo ratings yet
- 282-286 DR AkhaDocument5 pages282-286 DR AkhaBompi BamNo ratings yet
- High Risk of Coagulopathy Among Type-2 Diabetes Mellitus Clients at A Municipal Hospital in GhanaDocument7 pagesHigh Risk of Coagulopathy Among Type-2 Diabetes Mellitus Clients at A Municipal Hospital in GhanaLovi AnaNo ratings yet
- Influence of Triglycerides On Other Plasma Lipids in Middle-Aged Men Intended For Hypolipidaemic TreatmentDocument6 pagesInfluence of Triglycerides On Other Plasma Lipids in Middle-Aged Men Intended For Hypolipidaemic TreatmentPatrisia HallaNo ratings yet
- Gloomy LifeDocument6 pagesGloomy LifeLanna HarumiyaNo ratings yet
- 7 FFCDocument8 pages7 FFCHow to youNo ratings yet
- Compaison of SgotDocument4 pagesCompaison of SgotPournima WaghmareNo ratings yet
- Homocysteine and Markers of Coagulation and Endothelial Cell ActivationDocument7 pagesHomocysteine and Markers of Coagulation and Endothelial Cell ActivationMaya RustamNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 8: UrologyFrom EverandComplementary and Alternative Medical Lab Testing Part 8: UrologyRating: 3 out of 5 stars3/5 (1)
- Mayo Clinic Proceedings: Critical Glucose Control: The Devil Is in The DetailsDocument4 pagesMayo Clinic Proceedings: Critical Glucose Control: The Devil Is in The DetailstfurrahmanNo ratings yet
- HypertensionDocument7 pagesHypertensionrohayatjohnNo ratings yet
- 2010 ACE Gene MJMHS 2010Document6 pages2010 ACE Gene MJMHS 2010dvckpjuNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 3: CardiologyFrom EverandComplementary and Alternative Medical Lab Testing Part 3: CardiologyRating: 1 out of 5 stars1/5 (1)
- PDML Article1Document4 pagesPDML Article1kingdeyNo ratings yet
- Peran M Pada TikusDocument8 pagesPeran M Pada TikusShampuy ShampuyNo ratings yet
- R230C But Not 565C - T VariantDocument11 pagesR230C But Not 565C - T VariantRogelio MoscosoNo ratings yet
- Background/PurposeDocument4 pagesBackground/Purposeevi gustia kesumaNo ratings yet
- The Influence of Spleen On Portal HemodynamicsDocument1 pageThe Influence of Spleen On Portal HemodynamicsdenisegmeloNo ratings yet
- Clinical research shows rosuvastatin more effective than atorvastatin for metabolic syndromeDocument9 pagesClinical research shows rosuvastatin more effective than atorvastatin for metabolic syndromeSohail AhmedNo ratings yet
- BR J Haematol - 2007 - Vasavda - The Linear Effects of Thalassaemia The UGT1A1 and HMOX1 Polymorphisms On CholelithiasisDocument8 pagesBR J Haematol - 2007 - Vasavda - The Linear Effects of Thalassaemia The UGT1A1 and HMOX1 Polymorphisms On CholelithiasisJordan NGOUNENo ratings yet
- Montserrat Creus, Ramon Deulofeu, Joana Pe Ñ Arrubia, Francisco Carmona and Juan BalaschDocument7 pagesMontserrat Creus, Ramon Deulofeu, Joana Pe Ñ Arrubia, Francisco Carmona and Juan BalaschMecineanu ElenaNo ratings yet
- Association Of Tnf-Α And Uric Acid In Women With Pre-EclampsiaDocument5 pagesAssociation Of Tnf-Α And Uric Acid In Women With Pre-EclampsiaihdinzNo ratings yet
- Assessment of α1antitrypsin and α2macroglobulin levels in obese patientsDocument5 pagesAssessment of α1antitrypsin and α2macroglobulin levels in obese patientsAnnisa SufiNo ratings yet
- Article 03 PDFDocument4 pagesArticle 03 PDFFitria Dhenok BerAkziNo ratings yet
- Dia Care 1981 Welborn 616 9Document4 pagesDia Care 1981 Welborn 616 9godeberta18No ratings yet
- Hemostatic Changes in Active Pulmonary TuberculosisDocument6 pagesHemostatic Changes in Active Pulmonary Tuberculosisdvt nsNo ratings yet
- IL 18 in Diabetic Patients With and Without Coronary AtherosclerosisDocument5 pagesIL 18 in Diabetic Patients With and Without Coronary AtherosclerosisTenta Hartian HendyatamaNo ratings yet
- Leucocyte Differential Count May Predict Risk of Pregnancy Induced HypertensionDocument10 pagesLeucocyte Differential Count May Predict Risk of Pregnancy Induced Hypertensionhypebeast dopeNo ratings yet
- Macroangipatia DiabeticaDocument6 pagesMacroangipatia DiabeticaMarcos Chusin MontesdeocaNo ratings yet
- Atherogenic Dyslipidemia in Patients With Established Coronary Artery DiseaseDocument6 pagesAtherogenic Dyslipidemia in Patients With Established Coronary Artery DiseasebilahalvirayuNo ratings yet
- Lipid and Inflammatory Biomarkers and Kidney Function Decline in Type 2 DiabetesDocument5 pagesLipid and Inflammatory Biomarkers and Kidney Function Decline in Type 2 Diabetesannaafia69969No ratings yet
- 10.1515 - CCLM 2023 7044Document112 pages10.1515 - CCLM 2023 7044sfendri17No ratings yet
- Detection of Some Antioxidant Markers in Saliva of Patients With Beta Thalassemia MajorDocument11 pagesDetection of Some Antioxidant Markers in Saliva of Patients With Beta Thalassemia MajorReshmaa RajendranNo ratings yet
- Order - 523187 - Main Document With Abstract - TRACKED - REVISEDDocument12 pagesOrder - 523187 - Main Document With Abstract - TRACKED - REVISEDAn MNo ratings yet
- AMADEO Full PaperDocument6 pagesAMADEO Full PaperAnggraeni PermatasariNo ratings yet
- Sodium and Potassium Intake in Overweight And.596Document2 pagesSodium and Potassium Intake in Overweight And.596jackie funtanillaNo ratings yet
- Serum Ischemia Modified Albumin, Fibrinogen, HSCRP in DMT2 With and Without HypertensionDocument9 pagesSerum Ischemia Modified Albumin, Fibrinogen, HSCRP in DMT2 With and Without HypertensionMarcellia AngelinaNo ratings yet
- Hypertension Prevalence, Awareness, Control and Association With Metabolic Abnormalities in The San Marino Population: The SMOOTH StudyDocument7 pagesHypertension Prevalence, Awareness, Control and Association With Metabolic Abnormalities in The San Marino Population: The SMOOTH StudyIndah SundariNo ratings yet
- 1471 2261 5 7 PDFDocument10 pages1471 2261 5 7 PDFAfifah Raisa HalimNo ratings yet
- Factores Predict Ores en NASHDocument7 pagesFactores Predict Ores en NASHkukito77No ratings yet
- Anti-Inflammatory and Metabolic Effects of Candesartan in Hypertensive PatientsDocument5 pagesAnti-Inflammatory and Metabolic Effects of Candesartan in Hypertensive PatientsBarbara Sakura RiawanNo ratings yet
- HOMA Medicion EJIM2003Document6 pagesHOMA Medicion EJIM2003Dr Dart05No ratings yet
- Paper Title: (16 Bold)Document9 pagesPaper Title: (16 Bold)vegeto portmanNo ratings yet
- IOSR Journal of Pharmacy (IOSRPHR)Document6 pagesIOSR Journal of Pharmacy (IOSRPHR)IOSR Journal of PharmacyNo ratings yet
- Original Article Evaluation of Dyslipidaemia in Type 2 Diabetes Mellitus PatientsDocument6 pagesOriginal Article Evaluation of Dyslipidaemia in Type 2 Diabetes Mellitus PatientsEnvhy AmaliaNo ratings yet
- Research Journal of Pharmaceutical, Biological and Chemical SciencesDocument9 pagesResearch Journal of Pharmaceutical, Biological and Chemical SciencesMuhammad ZubaidiNo ratings yet
- Hyperfibrinogenemia Predicts Vascular Risk in DiabetesDocument6 pagesHyperfibrinogenemia Predicts Vascular Risk in DiabetesHeru MurdiantoNo ratings yet
- GoutDocument13 pagesGoutGanesa P. D. KurniawanNo ratings yet
- Effects of Cinacalcet on CV Risk, Fractures & QoL in SHPTDocument8 pagesEffects of Cinacalcet on CV Risk, Fractures & QoL in SHPTannarchyNo ratings yet
- Serum Uric AcidDocument7 pagesSerum Uric AcidAnonymous ceYk4p4No ratings yet
- IV Abra DineDocument6 pagesIV Abra Dineong251183No ratings yet
- SIS Semarang Tuition FeesDocument1 pageSIS Semarang Tuition Feesong251183No ratings yet
- Initiating Basal Insulin: Dr. Miftahurachman, Sppd-Kemd, M.Kes, FinasimDocument58 pagesInitiating Basal Insulin: Dr. Miftahurachman, Sppd-Kemd, M.Kes, Finasimong251183No ratings yet
- The Role of Insulin Premix 50 in DM Type 2 Management DR OnggoDocument31 pagesThe Role of Insulin Premix 50 in DM Type 2 Management DR Onggoong251183No ratings yet
- SubaruDocument10 pagesSubaruong251183No ratings yet
- Freeletics Workout Program - ExercisesDocument1 pageFreeletics Workout Program - Exercisesddaarreenn100% (4)
- Avrist Basic GuardDocument5 pagesAvrist Basic Guardong251183No ratings yet
- Brosur Prime 88Document2 pagesBrosur Prime 88ong251183No ratings yet
- Avrist Medi GuardDocument6 pagesAvrist Medi Guardong251183No ratings yet
- Clinical GuidelinesDocument8 pagesClinical Guidelinesong251183No ratings yet
- 00006Document12 pages00006ong251183No ratings yet
- 2013 ACCF AHA Guideline For The Management of ST-Elevation Myocardial Infarction - Executive SummaryDocument51 pages2013 ACCF AHA Guideline For The Management of ST-Elevation Myocardial Infarction - Executive Summaryong251183No ratings yet
- 1 s2.0 S088394411200322X Main PDFDocument5 pages1 s2.0 S088394411200322X Main PDFong251183No ratings yet
- Copd Power PointDocument33 pagesCopd Power PointRININo ratings yet
- Uric Acid, HyperDocument20 pagesUric Acid, HyperAlpascaFirdausNo ratings yet
- 2015 GOLD - Pocket Guide To COPD Diagnosis, Management and PreventionDocument32 pages2015 GOLD - Pocket Guide To COPD Diagnosis, Management and PreventionblueicelandNo ratings yet
- Cardiology BrochureDocument2 pagesCardiology Brochureong251183No ratings yet
- Uric Acid, HyperDocument20 pagesUric Acid, HyperAlpascaFirdausNo ratings yet
- 1 s2.0 S0735109714621021 MainDocument1 page1 s2.0 S0735109714621021 Mainong251183No ratings yet
- Current Prognosis Biomarker in BCDocument18 pagesCurrent Prognosis Biomarker in BCong251183No ratings yet
- 03 Chemo PrincDocument17 pages03 Chemo PrincMareeze HattaNo ratings yet
- Nutrition, Metabolism & Cardiovascular DiseasesDocument6 pagesNutrition, Metabolism & Cardiovascular Diseasesong251183No ratings yet
- Advances in Techniques of Testing Mycobacterial Drug Sensitivity, and The Use of Sensitivity Test in Tuberculosis Control ProgramsDocument23 pagesAdvances in Techniques of Testing Mycobacterial Drug Sensitivity, and The Use of Sensitivity Test in Tuberculosis Control Programsong251183No ratings yet
- An Integrative Genomic and Proteomic Analysis ofDocument9 pagesAn Integrative Genomic and Proteomic Analysis ofong251183No ratings yet
- Rapid Molecular Detection of Tuberculosis and Rifampicin ResistanceDocument11 pagesRapid Molecular Detection of Tuberculosis and Rifampicin Resistanceong251183No ratings yet
- Test AplotDocument1 pageTest AplotOnggo WiliyantoNo ratings yet
- Evaluation of COBAS TaqMan (R) MTB PCR For The Detection of Mycobacterium TuberculosisDocument4 pagesEvaluation of COBAS TaqMan (R) MTB PCR For The Detection of Mycobacterium Tuberculosisong251183No ratings yet
- Test AplotDocument1 pageTest AplotOnggo WiliyantoNo ratings yet
- An Update On The Pathogenesis of DiabetesDocument12 pagesAn Update On The Pathogenesis of DiabetesAmalia Elena BulanceaNo ratings yet
- Test AplotDocument1 pageTest AplotOnggo WiliyantoNo ratings yet
- Blood Group SerologyDocument89 pagesBlood Group SerologynelsonlaizerNo ratings yet
- 1-2 Hemostasis PhysiologyDocument48 pages1-2 Hemostasis PhysiologyHussein Al Saedi100% (2)
- Why Some Jehovah's Witnesses Accept BloodDocument6 pagesWhy Some Jehovah's Witnesses Accept BloodsirjsslutNo ratings yet
- Husmhema-Upt STM C1Document17 pagesHusmhema-Upt STM C1zakwanmustafaNo ratings yet
- Hematologic Disorders NCLEXDocument15 pagesHematologic Disorders NCLEXPotchiee PfizerNo ratings yet
- HEMA-Iron Deficiency Anemia & MegaloBalstic Anemia DRA CRUZDocument5 pagesHEMA-Iron Deficiency Anemia & MegaloBalstic Anemia DRA CRUZShams JailaniNo ratings yet
- Dr. HalimDocument2 pagesDr. HalimmembermemNo ratings yet
- D-Dimer PregnancyDocument5 pagesD-Dimer PregnancyKristabella GianinaNo ratings yet
- Body Fluids and CirculatoinDocument34 pagesBody Fluids and CirculatoinPrasmita BeheraNo ratings yet
- Online Assignment 5Document4 pagesOnline Assignment 5dia diaNo ratings yet
- Mathematical Models for Drug Diffusion Through Blood and TissueDocument5 pagesMathematical Models for Drug Diffusion Through Blood and TissueJuan Andres Bueno HortuaNo ratings yet
- Rab297cen - Yumizen H500 OT Daily Guide PDFDocument42 pagesRab297cen - Yumizen H500 OT Daily Guide PDFZhafira Afsheen Niesa100% (2)
- Mechanisms of Hemostasis - Contributions of Platelets, Coagulation Factors, and The Vessel WallDocument25 pagesMechanisms of Hemostasis - Contributions of Platelets, Coagulation Factors, and The Vessel WallelhierofanteNo ratings yet
- Biology Notes Chpter 10Document8 pagesBiology Notes Chpter 10Wan HasliraNo ratings yet
- The Human Body (Test in English)Document23 pagesThe Human Body (Test in English)Martina Sofia Oviedo LencinasNo ratings yet
- SCIENCE (Art Integrated Activity) Roll No. 1 To 5Document15 pagesSCIENCE (Art Integrated Activity) Roll No. 1 To 5Abhinav Kumar SinghNo ratings yet
- Basti KarmukataDocument31 pagesBasti KarmukataAkshataNo ratings yet
- Clinical Haematology AtlasDocument145 pagesClinical Haematology AtlasAnna100% (3)
- Understanding Thalassemia: Causes, Types and SymptomsDocument13 pagesUnderstanding Thalassemia: Causes, Types and SymptomsririNo ratings yet
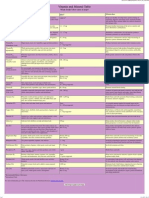
- Vitamin and Mineral TABLEDocument1 pageVitamin and Mineral TABLEHibozoNo ratings yet
- Physiological Effects of YogaDocument2 pagesPhysiological Effects of YogaNimesh Shah100% (1)
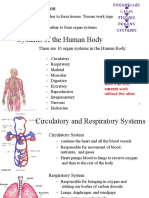
- Systems of The Human Body: OrganizationDocument10 pagesSystems of The Human Body: OrganizationCatherine Lagario Renante100% (1)
- Acute Hypercapnic Respiratory Failure Associated With HemodialysisDocument3 pagesAcute Hypercapnic Respiratory Failure Associated With HemodialysisMahmoud DiaaNo ratings yet
- Neonatal Polycythemia and HyperviscosityDocument8 pagesNeonatal Polycythemia and HyperviscosityToto HandayonoNo ratings yet
- SC003 1 Order of Draw WebsiteDocument3 pagesSC003 1 Order of Draw WebsitemariamNo ratings yet
- ACT Vs aPTTDocument2 pagesACT Vs aPTTSagar JethwaNo ratings yet
- Unit 2Document7 pagesUnit 2Nguyen CuongNo ratings yet
- Downloaded by Success Groups HF: AnswersDocument27 pagesDownloaded by Success Groups HF: AnswersMoh AmedNo ratings yet
- Stars Academy Lahore: Stars Entry Test SystemDocument2 pagesStars Academy Lahore: Stars Entry Test SystemMemoona GullNo ratings yet
- Blood Transfusions - TGH Policies & ProceduresDocument4 pagesBlood Transfusions - TGH Policies & ProceduresMark Anthony FranciscoNo ratings yet