You might also like
- Dermatosa Vesiko BulosaDocument14 pagesDermatosa Vesiko BulosaSyahrul Hamidi NasutionNo ratings yet
- DM Hiperestesia 4 PDFDocument6 pagesDM Hiperestesia 4 PDFSyahrul Hamidi NasutionNo ratings yet
- Nutrition, Diabetes and Tuberculosis in The Epidemiological TransitionDocument7 pagesNutrition, Diabetes and Tuberculosis in The Epidemiological TransitionSyahrul Hamidi NasutionNo ratings yet
- EvaluationDocument7 pagesEvaluationSyahrul Hamidi NasutionNo ratings yet
- Relationship Between Computed Tomography Findings and Nutritional Status in Elderly Patients With Pulmonary TuberculosisDocument6 pagesRelationship Between Computed Tomography Findings and Nutritional Status in Elderly Patients With Pulmonary TuberculosisSyahrul Hamidi NasutionNo ratings yet
- NIH Public Access: Author ManuscriptDocument10 pagesNIH Public Access: Author ManuscriptSyahrul Hamidi NasutionNo ratings yet
- Research Paper: ISSN 0189-6016©2009Document6 pagesResearch Paper: ISSN 0189-6016©2009Syahrul Hamidi NasutionNo ratings yet
- AJTCAM0701 0079jkjlkDocument6 pagesAJTCAM0701 0079jkjlkSyahrul Hamidi NasutionNo ratings yet
- AFHS0901 0040lkDocument6 pagesAFHS0901 0040lkSyahrul Hamidi NasutionNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- TRS - 2003.full - Crocodyliform Biogeography During The CretaceousDocument7 pagesTRS - 2003.full - Crocodyliform Biogeography During The CretaceousKanekoNo ratings yet
- Antibody Responses To Minor Histocompatibility Antigens After Solid Organ TransplantationDocument5 pagesAntibody Responses To Minor Histocompatibility Antigens After Solid Organ TransplantationBruna VoroniukNo ratings yet
- Hsslive XI Zoology 05 Digestion and AsorptionDocument15 pagesHsslive XI Zoology 05 Digestion and AsorptionbnairNo ratings yet
- Eoc Biology Rview Packet 2012-2013Document48 pagesEoc Biology Rview Packet 2012-2013api-282682755No ratings yet
- Certificate of Analysis No.: 1927745: CustomerDocument2 pagesCertificate of Analysis No.: 1927745: CustomerDimitris KNo ratings yet
- Revista - BJSM - Price Vs Police. PRICE Needs Updating, Should We Call The POLICE?Document3 pagesRevista - BJSM - Price Vs Police. PRICE Needs Updating, Should We Call The POLICE?Giancarlo Gardella MartínezNo ratings yet
- Irjet V9i1124Document5 pagesIrjet V9i1124BALAJINo ratings yet
- An Introduction To: The Respiratory SystemDocument22 pagesAn Introduction To: The Respiratory SystemSHANJIDA ALI RIANo ratings yet
- Personality DevelopmentDocument25 pagesPersonality DevelopmentmonishaNo ratings yet
- (Gardner) - (Snustad) Kontrol Genetik Respon ImunDocument21 pages(Gardner) - (Snustad) Kontrol Genetik Respon ImunFAUZI IBNUNo ratings yet
- Management of Diabetic KetoacidosisDocument4 pagesManagement of Diabetic Ketoacidosiscarla jazmin cortes rodriguezNo ratings yet
- Executive Summary: Intended Goals of SequencingDocument1 pageExecutive Summary: Intended Goals of SequencingBrahim JabbaneNo ratings yet
- IFAP Matrice D Import TAXO I Fap V12 31082020Document1,426 pagesIFAP Matrice D Import TAXO I Fap V12 31082020jamiNo ratings yet
- Food Enzymology: FD-206 Spring Semester 2021 Second Year Food EngineeringDocument25 pagesFood Enzymology: FD-206 Spring Semester 2021 Second Year Food EngineeringSahar Batool QaziNo ratings yet
- H O P E - 2-Module-2Document12 pagesH O P E - 2-Module-2kmpguarin.tshsNo ratings yet
- Allergic ConjunctivitisDocument16 pagesAllergic ConjunctivitisJose Antonio Fuentes VegaNo ratings yet
- B001 Arihant PDFDocument12 pagesB001 Arihant PDFmathclubNo ratings yet
- Qdoc - Tips Topnotch Supplement Pharmacology HandoutDocument57 pagesQdoc - Tips Topnotch Supplement Pharmacology HandoutShehana MusahariNo ratings yet
- Minerals Engineering: E.T. Pecina, L.F. Camacho, C.A. Herrera, D. MartínezDocument3 pagesMinerals Engineering: E.T. Pecina, L.F. Camacho, C.A. Herrera, D. MartínezMohsin ALiNo ratings yet
- Practice Prelim 3 Answer KeyDocument10 pagesPractice Prelim 3 Answer KeyEricaNo ratings yet
- QUS 104 Building ScienceDocument70 pagesQUS 104 Building ScienceOlagoke Habeeb Ademola100% (3)
- Old Earth History Book 1 - 5 Million To 750 B.C. - The AnnunakiDocument218 pagesOld Earth History Book 1 - 5 Million To 750 B.C. - The Annunaki123jump100% (11)
- Dissolved Oxygen and Aquatic Productivity LabDocument6 pagesDissolved Oxygen and Aquatic Productivity Labapi-235548856No ratings yet
- HemosIL APTT Brochure Rev2 May 07 PDFDocument4 pagesHemosIL APTT Brochure Rev2 May 07 PDFKath ONo ratings yet
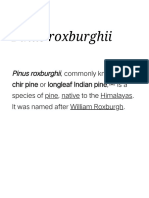
- Pinus Roxburghii - WikipediaDocument16 pagesPinus Roxburghii - WikipediaGener Habala NavarroNo ratings yet
- Fusion Diagnostics Lingad, Joselito Bohots: Sars-Cov-2 PCRDocument2 pagesFusion Diagnostics Lingad, Joselito Bohots: Sars-Cov-2 PCRjb lingadNo ratings yet
- Double CirculationDocument2 pagesDouble CirculationMonika KanojiaNo ratings yet
- 5 Paragraph Essay: Genetically Modified FoodDocument5 pages5 Paragraph Essay: Genetically Modified FoodAwais AliNo ratings yet
- Soal TOEIC Listening Ricky Dwi Agustyas (17020230056)Document9 pagesSoal TOEIC Listening Ricky Dwi Agustyas (17020230056)dwyas rickNo ratings yet