You might also like
- Tap Yourself FreeDocument134 pagesTap Yourself Freenguyenhavn100% (2)
- Mitchella Partridge Berry Materia Medica HerbsDocument3 pagesMitchella Partridge Berry Materia Medica HerbsAlejandra GuerreroNo ratings yet
- Surgical InstrumentsDocument4 pagesSurgical InstrumentsWafa L. AbdulrahmanNo ratings yet
- NUTRITIONAL AssessmentDocument46 pagesNUTRITIONAL AssessmentSonali Hazra0% (1)
- Nutritional AssessmentDocument6 pagesNutritional AssessmentReyna Mee AhiyasNo ratings yet
- Diet Survey (SUKRITI)Document37 pagesDiet Survey (SUKRITI)Juhi Neogi100% (1)
- Food Nutrients and NutritionDocument10 pagesFood Nutrients and NutritionAceNo ratings yet
- Nutrition and Diet Reviewer PrelimDocument5 pagesNutrition and Diet Reviewer PrelimKhrizztle Angel JamerlanNo ratings yet
- Test Bank For Nutrition 2nd Canadian Edition by SmolinDocument27 pagesTest Bank For Nutrition 2nd Canadian Edition by Smolina731968980100% (1)
- Diet For Infant and ToddlersDocument19 pagesDiet For Infant and ToddlersMelody B. Miguel100% (1)
- Nutrition Care Process Briefer CP OrientationDocument37 pagesNutrition Care Process Briefer CP OrientationAnni SholihahNo ratings yet
- MalnutritionDocument30 pagesMalnutritionbillyktoubatts100% (1)
- Dietary CalculationsDocument9 pagesDietary CalculationsV_RN100% (2)
- Nutrition in Infancy and ChildhoodDocument16 pagesNutrition in Infancy and ChildhoodThịnh Nguyễn PhúcNo ratings yet
- Casestudy 1Document6 pagesCasestudy 1api-240055755No ratings yet
- 10 - Nutrition During Infancy, Childhood and AdolescenceDocument45 pages10 - Nutrition During Infancy, Childhood and AdolescenceMaria Victoria A. PraxidesNo ratings yet
- Nutrition AssessmentDocument47 pagesNutrition AssessmentMohamed F. Nada100% (6)
- Nutritional Assessment Methods SummaryDocument45 pagesNutritional Assessment Methods SummaryJrose CuerpoNo ratings yet
- Renal Computation AssessmentDocument7 pagesRenal Computation AssessmentKathlene GamitNo ratings yet
- NutrientsDocument8 pagesNutrientsderic100% (4)
- Nutritional Consideration in Infancy and Preschool YearsDocument44 pagesNutritional Consideration in Infancy and Preschool YearsZemy RaoNo ratings yet
- Nutrition From Preschool To Adolescence - M.SC - DAN - 2016Document128 pagesNutrition From Preschool To Adolescence - M.SC - DAN - 2016Ria KumarNo ratings yet
- MNT Case Study For IBSDocument7 pagesMNT Case Study For IBSRuihan LINo ratings yet
- Nutri Lect1-6Document68 pagesNutri Lect1-6Zharm MayNo ratings yet
- Nutritional AssessmentDocument34 pagesNutritional AssessmentEli Zza Koirala100% (2)
- Nutrition Powerpoint Week 2Document20 pagesNutrition Powerpoint Week 2Shaira Kheil TumolvaNo ratings yet
- Chapter 2 - The Health HistoryDocument5 pagesChapter 2 - The Health HistoryEmvie Loyd Pagunsan-Itable100% (1)
- Basics of Therapeutic Diets PDFDocument12 pagesBasics of Therapeutic Diets PDFFaith MarfilNo ratings yet
- Family Nursing Care Plan: (A Case Study of Paglingayen Family)Document9 pagesFamily Nursing Care Plan: (A Case Study of Paglingayen Family)Adrian MallarNo ratings yet
- NUTRITIONAL ASSESSMENT GUIDEDocument4 pagesNUTRITIONAL ASSESSMENT GUIDEShesly PhilominaNo ratings yet
- Laboratory No.2Document3 pagesLaboratory No.2Tricia Anne Sernicula RoqueNo ratings yet
- Nutrition concepts, macronutrients, malnutrition, and nutrient functionsDocument9 pagesNutrition concepts, macronutrients, malnutrition, and nutrient functionsJoshua PelicanoNo ratings yet
- Chapter-8 Turbine and Governor TestingDocument10 pagesChapter-8 Turbine and Governor Testingafru2000No ratings yet
- Basal Metabolic Rate and Factors that Affect Energy ExpenditureDocument14 pagesBasal Metabolic Rate and Factors that Affect Energy ExpenditureAnahgen RomeoNo ratings yet
- Childhood NutritionDocument7 pagesChildhood NutritionYessaminNo ratings yet
- Dietary Intake AssessmentDocument4 pagesDietary Intake AssessmentMary Mae BuellaNo ratings yet
- 4608 Eed 01Document29 pages4608 Eed 01NickNo ratings yet
- Nutrition: - . - and The Surgical Patient (Pre and Post Operative Nutrition)Document58 pagesNutrition: - . - and The Surgical Patient (Pre and Post Operative Nutrition)SanaSofiyahNo ratings yet
- Nutri Lec Syl Lab UsDocument11 pagesNutri Lec Syl Lab UsJacq CalaycayNo ratings yet
- Unit 2 Nutritional Consideration in Infancy and Preschool Years, Educational PlatformDocument51 pagesUnit 2 Nutritional Consideration in Infancy and Preschool Years, Educational Platformzia ullah100% (1)
- Chapter 1 - Nutrition and Diet TherapyDocument59 pagesChapter 1 - Nutrition and Diet TherapySami Ingles100% (1)
- NCM 105 Lec: Nutriton and Diet Therapy Project On Therapeutic DietsDocument15 pagesNCM 105 Lec: Nutriton and Diet Therapy Project On Therapeutic DietsVinz OñoNo ratings yet
- Types of Diet in HospitalDocument14 pagesTypes of Diet in HospitalSher Lee Ho100% (1)
- Assessment of Nutritional StatusDocument16 pagesAssessment of Nutritional StatusJaspreet SinghNo ratings yet
- Nurse Nutrition Study Guide Exam 3Document30 pagesNurse Nutrition Study Guide Exam 3Ek100% (1)
- Nutrition Unit IDocument158 pagesNutrition Unit IAnuchithra Radhakrishnan100% (2)
- Energy MetabolismDocument15 pagesEnergy Metabolismshannon c. lewisNo ratings yet
- Nutrition and MetabolismDocument9 pagesNutrition and MetabolismarunatejaNo ratings yet
- Nutri Lab 10Document38 pagesNutri Lab 10Carl Josef C. GarciaNo ratings yet
- Minerals and Water EssentialsDocument7 pagesMinerals and Water Essentialsmildred alidonNo ratings yet
- CHN1 LP 2 QuianoDocument27 pagesCHN1 LP 2 QuianoMargarette GeresNo ratings yet
- Assessment of Nutrional StatusDocument35 pagesAssessment of Nutrional StatusSnowe CheyenneNo ratings yet
- Nutrition Nursing: ProteinsDocument38 pagesNutrition Nursing: ProteinsAngelyka Nicole Bengco David100% (1)
- Anthropometry 130824161551 Phpapp02Document48 pagesAnthropometry 130824161551 Phpapp02cuckoo1234No ratings yet
- Practical DieteticsDocument30 pagesPractical DieteticsRohit SharmaNo ratings yet
- Nutrition Care PlanDocument10 pagesNutrition Care Planapi-486925921No ratings yet
- The Changing Nutritional Needs Across The Life CycleDocument24 pagesThe Changing Nutritional Needs Across The Life CycleFrance Dave CantorNo ratings yet
- Life CycleDocument40 pagesLife CycleMugdha Dabir-PathakNo ratings yet
- Introduction To Health & Nutrition: DR Syed Belal HassanDocument40 pagesIntroduction To Health & Nutrition: DR Syed Belal HassanSyed Belal HassanNo ratings yet
- Head To Toe AssessmentDocument56 pagesHead To Toe AssessmentmisshieNo ratings yet
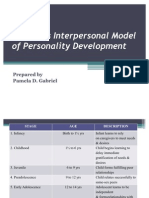
- Sullivan's Interpersonal Model and Erikson's Psychosocial StagesDocument8 pagesSullivan's Interpersonal Model and Erikson's Psychosocial StagesPamDavidGabrielNo ratings yet
- NUTRITION LIFESPAN MIDTERMSDocument20 pagesNUTRITION LIFESPAN MIDTERMSNathaniel PulidoNo ratings yet
- Rudwan Moh MCQsDocument337 pagesRudwan Moh MCQsmagde90No ratings yet
- NCP Form sp14 RepairedDocument6 pagesNCP Form sp14 Repairedapi-251349687No ratings yet
- Mercola Libro DietaDocument127 pagesMercola Libro DietaneuralterapianetNo ratings yet
- Rao-K-M-Tt - Diet and Nutritional Status of Women in IndiaDocument6 pagesRao-K-M-Tt - Diet and Nutritional Status of Women in IndiaRa ViLeo KUNo ratings yet
- Body Mass IndexDocument7 pagesBody Mass Indexnikhild77No ratings yet
- InTech-Impact of Globalization On Indian Technical Education SystemDocument24 pagesInTech-Impact of Globalization On Indian Technical Education Systemnikhild77No ratings yet
- Capital StructureDocument13 pagesCapital Structurenikhild77No ratings yet
- Fee Based Services11Document14 pagesFee Based Services11nikhild77No ratings yet
- UntitledDocument1 pageUntitlednikhild77No ratings yet
- Porters Five ForcesDocument4 pagesPorters Five Forcesnikhild77No ratings yet
- TCS Annual Report 2011-2012Document164 pagesTCS Annual Report 2011-2012akshay3912No ratings yet
- 4 Perfect CompetitionDocument5 pages4 Perfect Competitionnikhild77No ratings yet
- Washing Machines Case StudyDocument3 pagesWashing Machines Case Studynikhild77No ratings yet
- The Quill Vol. LVIII Issue 1 1-12Document12 pagesThe Quill Vol. LVIII Issue 1 1-12Yves Lawrence Ivan OardeNo ratings yet
- Myths of Greece and Rome PDFDocument247 pagesMyths of Greece and Rome PDFratheesh1981No ratings yet
- Contact GRRSB Team for InquiriesDocument2 pagesContact GRRSB Team for Inquiriesmsis81No ratings yet
- How Does Marijuana Affect The BrainDocument3 pagesHow Does Marijuana Affect The BrainWanNurAtikahNo ratings yet
- Project Data Collection & Risk ReportingDocument2 pagesProject Data Collection & Risk Reportinggambler yeagerNo ratings yet
- Whatever Happens, Happens For Something Good by MR SmileyDocument133 pagesWhatever Happens, Happens For Something Good by MR SmileyPrateek100% (3)
- Knowing Annelida: Earthworms, Leeches and Marine WormsDocument4 pagesKnowing Annelida: Earthworms, Leeches and Marine WormsCherry Mae AdlawonNo ratings yet
- Blood Group 3Document29 pagesBlood Group 3Hamirie JoshuaNo ratings yet
- Treasure Island Summary c#1-7Document4 pagesTreasure Island Summary c#1-7Great Wall Of FactsNo ratings yet
- News Writing April 2019Document39 pagesNews Writing April 2019Primrose EmeryNo ratings yet
- Schroedindiger Eqn and Applications3Document4 pagesSchroedindiger Eqn and Applications3kanchankonwarNo ratings yet
- Dahua Pfa130 e Korisnicko Uputstvo EngleskiDocument5 pagesDahua Pfa130 e Korisnicko Uputstvo EngleskiSaša CucakNo ratings yet
- Fund. of EnterpreneurshipDocument31 pagesFund. of EnterpreneurshipVarun LalwaniNo ratings yet
- Kendriya vidyalaya reading comprehension and grammar questionsDocument7 pagesKendriya vidyalaya reading comprehension and grammar questionsRaam sivaNo ratings yet
- Philip Rance EAH Philo of ByzantiumDocument3 pagesPhilip Rance EAH Philo of ByzantiumstoliNo ratings yet
- Pump Course Material Chapter 2Document16 pagesPump Course Material Chapter 2engr victorNo ratings yet
- Pembangkit ListrikDocument2 pagesPembangkit ListrikDede MulyamanNo ratings yet
- ARES SC4 Service Manual (HP-300UA)Document20 pagesARES SC4 Service Manual (HP-300UA)mike_net8903No ratings yet
- EVOLUTION Class Notes PPT-1-10Document10 pagesEVOLUTION Class Notes PPT-1-10ballb1ritikasharmaNo ratings yet
- Causes and Effects of PollutionDocument6 pagesCauses and Effects of PollutionNhư NgọcNo ratings yet
- Nitocote WP DDocument4 pagesNitocote WP DdaragNo ratings yet
- Is Revalida ExamDocument11 pagesIs Revalida ExamRodriguez, Jhe-ann M.No ratings yet
- Ebook Drugs and The Neuroscience of Behavior An Introduction To Psychopharmacology 2Nd Edition Prus Test Bank Full Chapter PDFDocument62 pagesEbook Drugs and The Neuroscience of Behavior An Introduction To Psychopharmacology 2Nd Edition Prus Test Bank Full Chapter PDFeffigiesbuffoonmwve9100% (10)
- ME 2141 - Complete ModuleDocument114 pagesME 2141 - Complete ModuleNICOLE ANN MARCELINONo ratings yet