You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
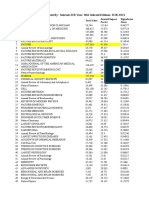
- Impact Factor 2021: List of Journals by Clarivate Analytics (JCR)Document264 pagesImpact Factor 2021: List of Journals by Clarivate Analytics (JCR)Medjahed AB100% (1)
- PHYSIOLOGY QuestionnaireDocument12 pagesPHYSIOLOGY QuestionnairePrasad KVVNo ratings yet
- Patient Satisfaction QuestionnaireDocument4 pagesPatient Satisfaction QuestionnairePrasad KVVNo ratings yet
- Garcinia CambogiaDocument29 pagesGarcinia CambogiaPrasad KVVNo ratings yet
- 35 SomeDocument12 pages35 SomePrasad KVVNo ratings yet
- Abel ThesisDocument74 pagesAbel ThesisPrasad KVVNo ratings yet
- The Structures of LifeDocument66 pagesThe Structures of LifePrasad KVVNo ratings yet
- GCLPDocument57 pagesGCLPkapindraNo ratings yet
- JCR Impact FactorDocument237 pagesJCR Impact FactorZakir UllahNo ratings yet
- Indian Couple Vacation in GoaDocument13 pagesIndian Couple Vacation in GoaPrasad KVVNo ratings yet
- P-660HN-T1A 3.40 Ed1Document324 pagesP-660HN-T1A 3.40 Ed1Rolyn Oswaldo Hernandez GamezNo ratings yet
- Healing Power WaterDocument6 pagesHealing Power WaterMaria BalochNo ratings yet
- Growth/ Height& Weight Chart of GirlsDocument1 pageGrowth/ Height& Weight Chart of GirlsPrasad KVVNo ratings yet
- Revised Pension Rules 1980Document329 pagesRevised Pension Rules 1980rameshmba2398100% (1)
- Medical Nutrition Therapy For Diabetes Type I & IIDocument10 pagesMedical Nutrition Therapy For Diabetes Type I & IIPrasad KVV100% (1)
- Chart 04chart 16rowth/ Height& Weight Chart of GirlsDocument1 pageChart 04chart 16rowth/ Height& Weight Chart of GirlsPrasad KVVNo ratings yet
- Diabetes Management at Camps For Children Wuth DiabetesDocument4 pagesDiabetes Management at Camps For Children Wuth DiabetesMicky SanjayaGameNo ratings yet
- Body Mass IndexDocument1 pageBody Mass IndexDanish AliNo ratings yet
- Diabetes Nutrition RecommendationsDocument18 pagesDiabetes Nutrition RecommendationsPrasad KVVNo ratings yet
- Akram AluDocument2 pagesAkram AluPrasad KVV0% (1)
- Remedies For PlanetsDocument3 pagesRemedies For PlanetsPrasad KVVNo ratings yet
- Passport Application Form GuideDocument2 pagesPassport Application Form GuidePhani BhupathirajuNo ratings yet
- Garlic Black Pepper Rasam RecipeDocument1 pageGarlic Black Pepper Rasam RecipePrasad KVVNo ratings yet
- Panchangam 13 - 14Document151 pagesPanchangam 13 - 14Vinod Sharma100% (1)
- Kokum RasamDocument1 pageKokum RasamPrasad KVVNo ratings yet
- Hyderabad ORR MapDocument1 pageHyderabad ORR MapIma Ricahards100% (1)
- GO Ms 901Document71 pagesGO Ms 901Badri NathNo ratings yet
- Chickpea DishDocument1 pageChickpea DishPrasad KVVNo ratings yet
- 03.MS WordDocument40 pages03.MS WordRichard ErasquinNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Pfizer, Inc: Company ValuationDocument15 pagesPfizer, Inc: Company ValuationPriyanka Jayanth DubeNo ratings yet
- Mimh Otc Timeline IIDocument5 pagesMimh Otc Timeline IInaren23No ratings yet
- WHO guidelines on quality risk managementDocument32 pagesWHO guidelines on quality risk managementanandhra2010No ratings yet
- Bob Beck's Lecture Notes: Doesn't Reflect AIDS' Early Strength Fight AIDSDocument30 pagesBob Beck's Lecture Notes: Doesn't Reflect AIDS' Early Strength Fight AIDSdocreader121100% (1)
- Chapter One: Market and Nonmarket Environments True/False QuestionsDocument15 pagesChapter One: Market and Nonmarket Environments True/False Questionschanyoung4951No ratings yet
- Psychotropic Drugs & ChildrenDocument6 pagesPsychotropic Drugs & ChildrenART.ASNNo ratings yet
- Antistax® Fresh Leg Gel: PSA Code of Ethics ReviewDocument3 pagesAntistax® Fresh Leg Gel: PSA Code of Ethics ReviewpharmacydailyNo ratings yet
- ATC 2014 GuidelinesDocument286 pagesATC 2014 GuidelinesSilvanaMedhatNo ratings yet
- Project Report TRIPSDocument18 pagesProject Report TRIPSAditya MayekarNo ratings yet
- GSK Placements Ppt-2012Document41 pagesGSK Placements Ppt-2012Saakshi WadhawanNo ratings yet
- Peer Review FormDocument3 pagesPeer Review FormHitesh VermaNo ratings yet
- The Aim of Medicine Is Not To Know The DiseaseDocument4 pagesThe Aim of Medicine Is Not To Know The DiseasekazchandranNo ratings yet
- Ethical Issues in Providing Pharmaceutical CareDocument7 pagesEthical Issues in Providing Pharmaceutical CareXee JayNo ratings yet
- HR - Informed Consent Form TemplateDocument9 pagesHR - Informed Consent Form TemplateHRCNo ratings yet
- Clinical Research BrochureDocument8 pagesClinical Research BrochureBen TennisonNo ratings yet
- DR - Reddy'S Laboratories LTD Hyderabad: Study On Employee Job Satisfaction ATDocument104 pagesDR - Reddy'S Laboratories LTD Hyderabad: Study On Employee Job Satisfaction ATlakshmanlakhsNo ratings yet
- Establishing Hold-Time Expiry of Manufacturing Process Solutions and The Use of Water Activity As A Microbial Growth PredictorDocument6 pagesEstablishing Hold-Time Expiry of Manufacturing Process Solutions and The Use of Water Activity As A Microbial Growth Predictorshah777No ratings yet
- Going To Pot by William Bennett and Robert WhiteDocument12 pagesGoing To Pot by William Bennett and Robert WhiteHBG Nashville0% (1)
- Role of FDA in Guiding Drug Development: Carl PeckDocument62 pagesRole of FDA in Guiding Drug Development: Carl PeckPrem PisupatiNo ratings yet
- Tinpus FarmakoekonomiDocument6 pagesTinpus FarmakoekonomiYesi Widya IswariNo ratings yet
- Biohealth Plak Insti-2Document2 pagesBiohealth Plak Insti-2api-67201372No ratings yet
- Packaging Unwrapped 2011Document48 pagesPackaging Unwrapped 2011Guillaume DryNo ratings yet
- NFDN 1002Document1 pageNFDN 1002api-319331499No ratings yet
- Master's Program Guide for Pediatrics at Ain Shams UniversityDocument121 pagesMaster's Program Guide for Pediatrics at Ain Shams UniversityIslam El SamaloutyNo ratings yet
- Maternal Health Advocacy Messages - A Roadmap For SuccessDocument84 pagesMaternal Health Advocacy Messages - A Roadmap For SuccesspathglobalhealthNo ratings yet
- Pharmacy Management System: (Desktop Application)Document39 pagesPharmacy Management System: (Desktop Application)Anuj MishraNo ratings yet
- Perianesthesia Nursing Standards of Practice Jennifer J SmithDocument11 pagesPerianesthesia Nursing Standards of Practice Jennifer J Smithapi-239605726No ratings yet
- Pe 011 1 Pics GDP GuideDocument27 pagesPe 011 1 Pics GDP GuideBlank SermNo ratings yet
- Assessment and Emergency Management of The Acutely Agitated or Violent Adult - UpToDateDocument20 pagesAssessment and Emergency Management of The Acutely Agitated or Violent Adult - UpToDateImja94100% (1)
- Ciclesonide Review PDFDocument31 pagesCiclesonide Review PDFarielighNo ratings yet