You might also like
- Chicago Review Press NCLEX-PN Practice Test and ReviewFrom EverandChicago Review Press NCLEX-PN Practice Test and ReviewRating: 4 out of 5 stars4/5 (4)
- Maternity Evolve ExamDocument36 pagesMaternity Evolve Examfriendofnurse100% (26)
- Maternity Nclex RN ReviewDocument11 pagesMaternity Nclex RN ReviewKwai Browne100% (7)
- NCLEX Questions and AnswersDocument16 pagesNCLEX Questions and AnswersJoslyn Gross100% (3)
- Med SurgDocument179 pagesMed Surgvinwaleed100% (1)
- ACIDDocument2 pagesACIDRizMarie100% (2)
- Select All That Apply SATADocument58 pagesSelect All That Apply SATANicholas TagleNo ratings yet
- DDocument56 pagesDDarren Balbas100% (1)
- New Text DocumentDocument3 pagesNew Text DocumentTro Wact100% (1)
- Medical Surgical Nursing 7th Edition Ignatavicius Test BankDocument9 pagesMedical Surgical Nursing 7th Edition Ignatavicius Test Bankqocax0% (1)
- Blue Print Final Class Med Surg IIDocument9 pagesBlue Print Final Class Med Surg IIbaconhater100% (1)
- Med Surge 2 Mod 3 Study GuideDocument19 pagesMed Surge 2 Mod 3 Study GuideDirk Buckner100% (4)
- Nursing Nclex ExamDocument11 pagesNursing Nclex ExamDenisa Viviana MaroNo ratings yet
- Obstetric Questions: Please State Whether The Following Statements Are TRUE or FALSEDocument8 pagesObstetric Questions: Please State Whether The Following Statements Are TRUE or FALSEjulialeo90% (10)
- NCLEX PN Practice Exam Set I-VDocument56 pagesNCLEX PN Practice Exam Set I-Vaajo136No ratings yet
- Med Surge 2 Mod 1 CardiacDocument13 pagesMed Surge 2 Mod 1 CardiacDirk Buckner100% (2)
- Nclex Practice Exam Part1Document20 pagesNclex Practice Exam Part1stuffednurse40% (5)
- Med SurgDocument9 pagesMed SurgVanessaMUeller100% (1)
- DiarrheaDocument24 pagesDiarrheaash ashNo ratings yet
- DEAR TO NCLEX's HEART PDFDocument452 pagesDEAR TO NCLEX's HEART PDFrn msn100% (4)
- Ati Comp ExitDocument53 pagesAti Comp Exitpretty shiks100% (1)
- Med Surg ReviewDocument6 pagesMed Surg ReviewSabhi Sandhu75% (4)
- Nclex Questions - Medical Surgical NursingDocument15 pagesNclex Questions - Medical Surgical NursingRegine Gozo100% (1)
- 60 Item Medical Surgical Nursing : Musculoskeletal Examination AnswersDocument10 pages60 Item Medical Surgical Nursing : Musculoskeletal Examination AnswersApril Kirstin ChuaNo ratings yet
- HESI NCLEX Study Guide: Essential Tips, Normal Values, MedicationsDocument21 pagesHESI NCLEX Study Guide: Essential Tips, Normal Values, MedicationsCaitlin Elliott100% (2)
- Med Surg BulletsDocument35 pagesMed Surg Bulletscfournier1982No ratings yet
- Nclex EyesDocument9 pagesNclex EyesYoke W Khoo100% (1)
- Med-Surg HESI TOPICSDocument6 pagesMed-Surg HESI TOPICSjustjesko0l100% (3)
- NATIONAL COUNCIL LICENSURE EXAMINATION FOR REGISTERED NURSES (NCLEX-RN): Passbooks Study GuideFrom EverandNATIONAL COUNCIL LICENSURE EXAMINATION FOR REGISTERED NURSES (NCLEX-RN): Passbooks Study GuideNo ratings yet
- Hesi HintsDocument42 pagesHesi HintsJohn Thomas100% (2)
- NCLEX EndocrineDocument21 pagesNCLEX EndocrineChristopher Harris100% (7)
- Med Surg Final Exam MapDocument42 pagesMed Surg Final Exam MapAnais Hall-Garrison100% (1)
- View AnswersDocument4 pagesView AnswersFaith Levi Alecha AlferezNo ratings yet
- Testing - 2 NclexDocument12 pagesTesting - 2 NclexYoke W KhooNo ratings yet
- Testing - 2 NclexDocument12 pagesTesting - 2 NclexYoke W KhooNo ratings yet
- Endocrine Nclex QuestionsDocument9 pagesEndocrine Nclex QuestionsTiffany Fain Noles100% (1)
- Pest Control Risk Assessment Indoor and OutdoorDocument72 pagesPest Control Risk Assessment Indoor and OutdoorarmkarthickNo ratings yet
- Viral Exanthems: Sahara Tuazan AbonawasDocument75 pagesViral Exanthems: Sahara Tuazan AbonawasMarlon Cenabre Turaja100% (1)
- Medsurg ATIDocument7 pagesMedsurg ATIloveoverpride12% (17)
- Pediatric RemediationDocument5 pagesPediatric RemediationAlvin L. Rozier67% (3)
- Nclex PharmaDocument22 pagesNclex Pharmakennedy14344No ratings yet
- NCLEX Exam Cardiovascular Surgery CareDocument5 pagesNCLEX Exam Cardiovascular Surgery CareHeather ClemonsNo ratings yet
- Iggy Med Surg Test Bank Chapter 007Document10 pagesIggy Med Surg Test Bank Chapter 007Tracy Bartell100% (5)
- Unit 8 Med Surg Study Guide NursingDocument5 pagesUnit 8 Med Surg Study Guide Nursingatl_nurse_student100% (7)
- NCLEX2015Document61 pagesNCLEX2015Sara Pirman100% (2)
- NCLEX Success PrayerDocument377 pagesNCLEX Success Prayerjkrix100% (2)
- Chapter 35 - Ignatavicius Medical Surgical NursingDocument6 pagesChapter 35 - Ignatavicius Medical Surgical Nursinggrkpanygiri100% (4)
- Kriya For Balancing The ChakrasDocument5 pagesKriya For Balancing The ChakrasFedra Fox Cubeddu100% (2)
- Reviewer For The Board Exam Part 4Document12 pagesReviewer For The Board Exam Part 4jamchan100% (5)
- Reviewer For The Board Exam Part 1Document34 pagesReviewer For The Board Exam Part 1jamchan100% (7)
- Reviewer For The Board Exam Part 3Document14 pagesReviewer For The Board Exam Part 3jamchan89% (9)
- Emergency Preparedness Concepts Test BankDocument13 pagesEmergency Preparedness Concepts Test BankTyson Easo JonesNo ratings yet
- Quiz 2-Med Surg-Final Review QuestionsDocument4 pagesQuiz 2-Med Surg-Final Review QuestionsSarah Blockno100% (2)
- Pediatric HESI Review 2016Document9 pagesPediatric HESI Review 2016Brittany78% (9)
- Med SurgTest2Document17 pagesMed SurgTest2Becca Sanborn100% (2)
- NCLEX Study GuideDocument2 pagesNCLEX Study GuideLogin Nurse100% (1)
- Tubes NclexDocument3 pagesTubes NclexYoke W Khoo100% (1)
- Hesi v4 Sample 2015Document2 pagesHesi v4 Sample 2015james67% (3)
- MedSurg GIDocument4 pagesMedSurg GIZachary T HallNo ratings yet
- Pharm Review For Hesi From JanaDocument8 pagesPharm Review For Hesi From Janacheyenne.black5205100% (1)
- Fluid Electrolytes Acid Base BalanceDocument18 pagesFluid Electrolytes Acid Base BalanceVin Lorenzo Campbell100% (1)
- DO NOT Delegate What You Can EATDocument1 pageDO NOT Delegate What You Can EATMerlin JosephNo ratings yet
- NCLEX Helpful HintsDocument2 pagesNCLEX Helpful HintsJamie Antonini GrantNo ratings yet
- Anatomy and Physiology Digestive System GuideDocument214 pagesAnatomy and Physiology Digestive System Guideyisel56100% (6)
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideFrom EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideNo ratings yet
- Tubes NclexDocument3 pagesTubes NclexYoke W Khoo100% (1)
- Testing NclexDocument5 pagesTesting NclexYoke W KhooNo ratings yet
- Nclex Thyroid DisordersDocument5 pagesNclex Thyroid DisordersYoke W KhooNo ratings yet
- Pediatrics NclexDocument1 pagePediatrics NclexYoke W KhooNo ratings yet
- Nclex Reflexes and Their IndicationDocument1 pageNclex Reflexes and Their IndicationYoke W KhooNo ratings yet
- IV. Physical Assessment Norms Actual Findings Interpretation and Analysis General Appearance Posture / GaitDocument9 pagesIV. Physical Assessment Norms Actual Findings Interpretation and Analysis General Appearance Posture / GaitMarianne_Miraflo_154No ratings yet
- Spironolactone Class Indications: 25MG TAB, 50Mg Tab, 100Mg TabDocument2 pagesSpironolactone Class Indications: 25MG TAB, 50Mg Tab, 100Mg TabAhmad KusayiriNo ratings yet
- Resume 2019Document1 pageResume 2019api-316723361No ratings yet
- Chapter 8 ErgonomicsDocument18 pagesChapter 8 ErgonomicsAsif Rahman RaktimNo ratings yet
- Pelvic Floor Exercises in The Elderly Irmina Nahon1Document34 pagesPelvic Floor Exercises in The Elderly Irmina Nahon1Anonymous C7H7wS6No ratings yet
- Jeff Hooper ThesisDocument445 pagesJeff Hooper ThesisRan CarilloNo ratings yet
- A Review On Aleurites MoluccanaDocument18 pagesA Review On Aleurites Moluccanabharatkhurana85No ratings yet
- Joint InfectionsDocument10 pagesJoint InfectionsJPNo ratings yet
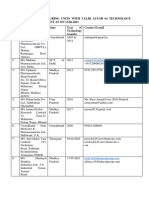
- List of Manufacturing Units With Valid Ayush 64 Technology Transfer Agreement As On 15.06.2021Document5 pagesList of Manufacturing Units With Valid Ayush 64 Technology Transfer Agreement As On 15.06.2021Sunira EnterprisesNo ratings yet
- Chapter 8 Spelling WordsDocument2 pagesChapter 8 Spelling Wordsapi-3705891No ratings yet
- Pre Employment Occupational Health FormDocument7 pagesPre Employment Occupational Health Formlinks2309No ratings yet
- Inspiring With Cystic FibrosisDocument2 pagesInspiring With Cystic FibrosisBeverlyHillsWeeklyNo ratings yet
- Grievously: News Item 9: EARTHQUAKE 2Document2 pagesGrievously: News Item 9: EARTHQUAKE 2roxana_boraNo ratings yet
- Nursing Comps Study GuideDocument15 pagesNursing Comps Study GuideforminskoNo ratings yet
- Drug Study AdalatDocument4 pagesDrug Study AdalatLea CelestialNo ratings yet
- References Style and Writing GuideDocument23 pagesReferences Style and Writing GuideHarshal SabaneNo ratings yet
- Permission To Attend Hockey DayDocument4 pagesPermission To Attend Hockey Dayapi-244287783No ratings yet
- FISIOGRAFT ENG Set 17 PDFDocument28 pagesFISIOGRAFT ENG Set 17 PDFmaxNo ratings yet
- Drug Release Kinetics ModelsDocument7 pagesDrug Release Kinetics ModelsSajid Khan SadozaiNo ratings yet
- Zocor (Simvastatin)Document3 pagesZocor (Simvastatin)E100% (1)
- Daftar Obat Slow Moving Dan Ed Rawat Inap Maret 2021Document8 pagesDaftar Obat Slow Moving Dan Ed Rawat Inap Maret 2021Vima LadipaNo ratings yet
- Review of Literature: MorphologyDocument38 pagesReview of Literature: MorphologyVaishu Gunalan0% (1)
- YOU IN SURGICAL - Product CatalogDocument222 pagesYOU IN SURGICAL - Product CatalogfarazNo ratings yet
- 64 Vital Nerve CentresDocument29 pages64 Vital Nerve CentresadinaNo ratings yet