You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Aslmualaikum WR WBDocument6 pagesAslmualaikum WR WBrantiadrianiNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- AbstractDocument10 pagesAbstractrantiadrianiNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Learn to Write the Letter C with Curved LinesDocument1 pageLearn to Write the Letter C with Curved LinesrantiadrianiNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Practice Tracing B Prek PDFDocument1 pagePractice Tracing B Prek PDFrantiadrianiNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Handbook: For Clinical Management of DengueDocument124 pagesHandbook: For Clinical Management of DengueraattaiNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- MRI in MTDocument13 pagesMRI in MTrantiadrianiNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Pang Imunopathogenesis Dss PDFDocument3 pagesPang Imunopathogenesis Dss PDFrantiadrianiNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- GipsDocument13 pagesGipsrantiadrianiNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Rajapakse Dengue ShockDocument9 pagesRajapakse Dengue ShockrantiadrianiNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- Practice Tracing D PrekDocument1 pagePractice Tracing D PrekrantiadrianiNo ratings yet
- Practice Tracing B Prek PDFDocument1 pagePractice Tracing B Prek PDFrantiadrianiNo ratings yet
- Practice Tracing e PrekDocument1 pagePractice Tracing e PrekrantiadrianiNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Daftar Pustaka RadiologiDocument1 pageDaftar Pustaka RadiologirantiadrianiNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Managing Immune Thrombocytopenic Purpura: An UpdateDocument7 pagesManaging Immune Thrombocytopenic Purpura: An UpdateApriliza RalasatiNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- 6 PDFDocument5 pages6 PDFUgaugaaNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Preterm Birth - WHO RecommendationDocument108 pagesPreterm Birth - WHO RecommendationBonifacius Bayu Erlangga KusumaNo ratings yet
- European ConsensusDocument19 pagesEuropean ConsensusEdgar Quelex VicenteNo ratings yet
- Daftar Pustaka Sepsis Tugas UjianDocument2 pagesDaftar Pustaka Sepsis Tugas UjianrantiadrianiNo ratings yet
- Eficacy Surfactant 2016Document13 pagesEficacy Surfactant 2016rantiadrianiNo ratings yet
- Cardiac Anomali ResearchDocument5 pagesCardiac Anomali ResearchrantiadrianiNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Pang Imunopathogenesis Dss PDFDocument3 pagesPang Imunopathogenesis Dss PDFrantiadrianiNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- YUVARAJAN-DeNGUE Pulmonal ComplicationDocument6 pagesYUVARAJAN-DeNGUE Pulmonal ComplicationrantiadrianiNo ratings yet
- Clinical Presenyation Dengue in ChildrenDocument4 pagesClinical Presenyation Dengue in ChildrenrantiadrianiNo ratings yet
- Shock Risk FactorDocument4 pagesShock Risk FactorrantiadrianiNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Devarajan, Dss DGN ArdsDocument4 pagesDevarajan, Dss DGN ArdsrantiadrianiNo ratings yet
- Role of Hematologic Scoring System in Early Diagnosis of Neonatal SepticemiaDocument6 pagesRole of Hematologic Scoring System in Early Diagnosis of Neonatal SepticemiarantiadrianiNo ratings yet
- Handbook: For Clinical Management of DengueDocument124 pagesHandbook: For Clinical Management of DengueraattaiNo ratings yet
- GipsDocument13 pagesGipsrantiadrianiNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- A Dede Ji 422017 Aj Mah 32627Document9 pagesA Dede Ji 422017 Aj Mah 32627rantiadrianiNo ratings yet
- Hematologic Scoring for Early Neonatal Sepsis DiagnosisDocument5 pagesHematologic Scoring for Early Neonatal Sepsis DiagnosisrantiadrianiNo ratings yet
- Basic Manicure: Level 2Document14 pagesBasic Manicure: Level 2Anonymous t5TDwdNo ratings yet
- Test in The Safety PDFDocument35 pagesTest in The Safety PDFJaber Al JafarNo ratings yet
- Immune Response ExplainedDocument34 pagesImmune Response ExplainedAtanas NaydenovNo ratings yet
- Pelvic Fracture (Case Presentation)Document36 pagesPelvic Fracture (Case Presentation)Arce A. CacalNo ratings yet
- Adult HIV Notes On GuidelinesDocument423 pagesAdult HIV Notes On GuidelinesJokerNo ratings yet
- The Social Impact of Covid-19Document1 pageThe Social Impact of Covid-19Trisha MaguikayNo ratings yet
- Odessa National Medical University: Surgical InfectionsDocument34 pagesOdessa National Medical University: Surgical InfectionsDrRajneesh ShastriNo ratings yet
- Thypoid FeverDocument6 pagesThypoid FeverRizki DickyNo ratings yet
- Notes - Sporozoa PDFDocument15 pagesNotes - Sporozoa PDFJezzah Mae CañeteNo ratings yet
- CSIR Model Test Paper 1Document12 pagesCSIR Model Test Paper 1Savitha ChellappanNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Naresa Community Resource Final PaperDocument6 pagesNaresa Community Resource Final Paperapi-342113680No ratings yet
- TreatmentDocument13 pagesTreatmentAnastasiafynnNo ratings yet
- A. Definition: Septic ShockDocument9 pagesA. Definition: Septic ShockKimberly Subade MandilagNo ratings yet
- Gas Gangrene: DR Mohammed Akbar KhanDocument89 pagesGas Gangrene: DR Mohammed Akbar KhanAkbar KhanNo ratings yet
- Ear, Nose and Throat (ENT) Infections Antibiotic GuidelinesDocument9 pagesEar, Nose and Throat (ENT) Infections Antibiotic GuidelinesAtta Muhammad MemonNo ratings yet
- Sericulture ManualDocument37 pagesSericulture ManualBabu Ram Panthi100% (10)
- MCQDocument9 pagesMCQpkm7929No ratings yet
- Anopheline Fauna, Hazaribag, JharkhandDocument4 pagesAnopheline Fauna, Hazaribag, Jharkhandmrazivbu23No ratings yet
- Adverse Events CTC A Ev 4Document42 pagesAdverse Events CTC A Ev 4fidodido2000No ratings yet
- Synonyms Egg Drop, Egg Drop Syndrome 76, EDS-76Document17 pagesSynonyms Egg Drop, Egg Drop Syndrome 76, EDS-76rahma tamren100% (1)
- Pacifc MMI Application Form PDFDocument6 pagesPacifc MMI Application Form PDFKaitaMahnNo ratings yet
- CDC GuidelinesDocument242 pagesCDC GuidelinesRao Rizwan ShakoorNo ratings yet
- Kebijakan Kanker ServiksDocument11 pagesKebijakan Kanker ServiksNur FajriyaNo ratings yet
- Points to Remember: Classification SystemsDocument10 pagesPoints to Remember: Classification SystemsANo ratings yet
- Dichotomous Key SampleDocument1 pageDichotomous Key SampleGerald ShouNo ratings yet
- Module 6 - Laboratory Investigation: Foodborne Disease Outbreak Investigation Team TrainingDocument44 pagesModule 6 - Laboratory Investigation: Foodborne Disease Outbreak Investigation Team TrainingrepyNo ratings yet
- Mycobacterium smegmatis Research OverviewDocument6 pagesMycobacterium smegmatis Research OverviewSalil ShauNo ratings yet
- Salivary GlandsDocument68 pagesSalivary GlandsTatiana Decuseară100% (1)
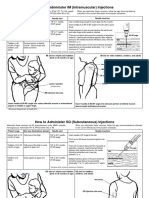
- Im SQ Admin PDFDocument2 pagesIm SQ Admin PDFAlvin JjNo ratings yet
- Briefing Note: Antimicrobial Resistance: An Emerging Water, Sanitation and Hygiene IssueDocument16 pagesBriefing Note: Antimicrobial Resistance: An Emerging Water, Sanitation and Hygiene IssueBoni MagtibayNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)