You might also like
- Discharge Delay in Acute Care Reasons and DeterminantsDocument9 pagesDischarge Delay in Acute Care Reasons and DeterminantsGabriela ObonNo ratings yet
- Peterson 2012Document5 pagesPeterson 2012Putri Rizky AmaliaNo ratings yet
- Impact of A Modified Nursing Handover ModelDocument9 pagesImpact of A Modified Nursing Handover ModelAngela NeriNo ratings yet
- Ebp PaperDocument35 pagesEbp Paperapi-654403621No ratings yet
- The Extent of Knowledge and Participation of The Staff Nurses On The Visual Infusion Phlebitis Program of Saint Anthony College HospitalDocument89 pagesThe Extent of Knowledge and Participation of The Staff Nurses On The Visual Infusion Phlebitis Program of Saint Anthony College HospitalWinj BudayNo ratings yet
- Malnutrition in Acute Care PatientsDocument19 pagesMalnutrition in Acute Care PatientsgabrielvadNo ratings yet
- The Utilization of Nursing Research in Extended CareDocument31 pagesThe Utilization of Nursing Research in Extended Careapi-285171922No ratings yet
- Emergency DepartmentDocument9 pagesEmergency DepartmentSarah Mae SanchezNo ratings yet
- Bronchiolitis - Nov 08Document8 pagesBronchiolitis - Nov 08Mark SosaNo ratings yet
- Clinical History-Taking and Physical Examination in Medical Practice in Africa: Still Relevant?Document4 pagesClinical History-Taking and Physical Examination in Medical Practice in Africa: Still Relevant?Asluf AmaanNo ratings yet
- Malnutrition in Acute Care Patients: A Narrative Review: Cathy Kubrak, Louise JensenDocument19 pagesMalnutrition in Acute Care Patients: A Narrative Review: Cathy Kubrak, Louise JensenchanchandilNo ratings yet
- Journal Presentation of Nisha LsDocument7 pagesJournal Presentation of Nisha LsANOOPVANo ratings yet
- Iefing The Value of Quality Malnutrition CareDocument5 pagesIefing The Value of Quality Malnutrition CareVelasquez LuisNo ratings yet
- Nurturing and Nourishing The Nurses Role in Nutritional CareDocument15 pagesNurturing and Nourishing The Nurses Role in Nutritional CareAgrista Yosita BaniNo ratings yet
- Association Between Emergency Department Length Of.10Document6 pagesAssociation Between Emergency Department Length Of.10mutu wonogiriNo ratings yet
- Desmarais 2015Document4 pagesDesmarais 2015Jesica DiazNo ratings yet
- NIH Public AccessDocument11 pagesNIH Public AccessDian WrwNo ratings yet
- Get Homework/Assignment DoneDocument6 pagesGet Homework/Assignment Donehomeworkping1No ratings yet
- 7 Clinical History Taking and Physical Examination in Medical Practice in AfricaDocument3 pages7 Clinical History Taking and Physical Examination in Medical Practice in AfricaStephanie CalleNo ratings yet
- Digest 4Document5 pagesDigest 4teguh triananda putraNo ratings yet
- ICU Family NeedsDocument14 pagesICU Family NeedsIstiqomahsejatiNo ratings yet
- Patient Perceptions of The Role of Nutrition For Pressure Ulcer Prevention in HospitalDocument7 pagesPatient Perceptions of The Role of Nutrition For Pressure Ulcer Prevention in HospitalSher UmarNo ratings yet
- Hospital Management SystemDocument6 pagesHospital Management SystemYohannes KefyalewNo ratings yet
- Pediatric Hospital Adherence To The Standard of Care For Acute GastroenteritisDocument9 pagesPediatric Hospital Adherence To The Standard of Care For Acute GastroenteritisAnggi Apriansyah PNo ratings yet
- Journal For MEdical WardDocument8 pagesJournal For MEdical WardValcrist BalderNo ratings yet
- Nurse-Directed Interventions To Reduce Catheter-Associated Urinary Tract InfectionsDocument10 pagesNurse-Directed Interventions To Reduce Catheter-Associated Urinary Tract InfectionsAngernani Trias WulandariNo ratings yet
- Literature Review DeliriumDocument7 pagesLiterature Review Deliriumafmzadevfeeeat100% (1)
- Kerr - Framework ED HandoverDocument11 pagesKerr - Framework ED HandoverNadia RizkinaNo ratings yet
- Early MobilizationDocument9 pagesEarly MobilizationBlake BoggenpoelNo ratings yet
- Maria Adorno Week 5 RUADocument6 pagesMaria Adorno Week 5 RUAMaria AdornoNo ratings yet
- Awareness of Medical Orders For Life Sustaining Treatmen - 2016 - Journal of PaiDocument1 pageAwareness of Medical Orders For Life Sustaining Treatmen - 2016 - Journal of PaiDipendra PratapNo ratings yet
- Wagg, Duckett To What Extent Are National Guidelines For The Management of Urinary Incontinence in Women AdheredDocument9 pagesWagg, Duckett To What Extent Are National Guidelines For The Management of Urinary Incontinence in Women Adheredsantivasa74No ratings yet
- 1 s2.0 S0197457212000675 Main PDFDocument8 pages1 s2.0 S0197457212000675 Main PDFRio Ady IrwansyahNo ratings yet
- Baby Hug Trial - Hidroxyrea For Sickle Cell Disease in ChildrenDocument8 pagesBaby Hug Trial - Hidroxyrea For Sickle Cell Disease in ChildrenTiago UchôaNo ratings yet
- Jurnal IDocument24 pagesJurnal IAgustin LindaNo ratings yet
- Professional Med J Q 2013 20 6 973 980Document8 pagesProfessional Med J Q 2013 20 6 973 980Vikram AripakaNo ratings yet
- Renal Health Advocacy For Nurses in La Union 1325915359Document13 pagesRenal Health Advocacy For Nurses in La Union 1325915359Rizki MatondangNo ratings yet
- Clinical Nursing Research: Patients' Perceptions of Hospital Discharge Informational ContentDocument21 pagesClinical Nursing Research: Patients' Perceptions of Hospital Discharge Informational ContentLivia MendonçaNo ratings yet
- ICU to Ward Patient Transfer Study ProtocolDocument7 pagesICU to Ward Patient Transfer Study ProtocolDiana SinuhajiNo ratings yet
- 117-jhn 12314Document12 pages117-jhn 12314Tolga CoşkunNo ratings yet
- ABDOME AGUDO IDOSO Modified Hospital Elder Life Program Effects On Abdominal Surgery Patients.Document8 pagesABDOME AGUDO IDOSO Modified Hospital Elder Life Program Effects On Abdominal Surgery Patients.Joao FonsecaNo ratings yet
- Anita Atwal - Nurses Perceptions of Discharge Planning in Acute Health CareDocument9 pagesAnita Atwal - Nurses Perceptions of Discharge Planning in Acute Health CareHaryaman JustisiaNo ratings yet
- Transitional CaresDocument11 pagesTransitional CaresEddNo ratings yet
- Decreasing Hospital Readmissions in Ileostomy PatientsDocument6 pagesDecreasing Hospital Readmissions in Ileostomy PatientsMEKSELINA KALENDERNo ratings yet
- Chapter-1-STEM-11-4-Group-1 EditedDocument12 pagesChapter-1-STEM-11-4-Group-1 EditedChristianzzz CalibsNo ratings yet
- Hospital Inpatientsõ Experiences of Access To Food: A Qualitative Interview and Observational StudyDocument10 pagesHospital Inpatientsõ Experiences of Access To Food: A Qualitative Interview and Observational StudyTolga CoşkunNo ratings yet
- Delayed Diagnosis For Undescended Testes: CKS, S V, R K, SNDocument2 pagesDelayed Diagnosis For Undescended Testes: CKS, S V, R K, SNJason FletcherNo ratings yet
- Chahine 2008Document8 pagesChahine 2008jumabarrientosNo ratings yet
- Contributing Factors To Hemodialysis Adherence in Aceh, Indonesia - ScienceDirectDocument6 pagesContributing Factors To Hemodialysis Adherence in Aceh, Indonesia - ScienceDirectlaamaghfirohNo ratings yet
- Journal Pre-Proof: Archives of Physical Medicine and RehabilitationDocument31 pagesJournal Pre-Proof: Archives of Physical Medicine and RehabilitationJuan David Hernández CifuentesNo ratings yet
- Pa Shik Anti 2012Document8 pagesPa Shik Anti 2012Irfan FauziNo ratings yet
- Association of Anorectal Malformation and Intestinal MalrotationDocument6 pagesAssociation of Anorectal Malformation and Intestinal MalrotationMirza RisqaNo ratings yet
- Eliza Final DissertationDocument58 pagesEliza Final DissertationCharlesNo ratings yet
- Partial Hip Replacement EditedDocument68 pagesPartial Hip Replacement EditedESTHER ROSE ZACALNo ratings yet
- Handover ERDocument12 pagesHandover EREros CuestaNo ratings yet
- Article: Risk Factors Associated With Acute Pyelonephritis in Healthy WomenDocument9 pagesArticle: Risk Factors Associated With Acute Pyelonephritis in Healthy WomenshahidmodarresNo ratings yet
- The Importance of Health Literacy in Physiotherapy Practice: Andrew M Briggs and Joanne E JordanDocument3 pagesThe Importance of Health Literacy in Physiotherapy Practice: Andrew M Briggs and Joanne E JordanMhmd IrakyNo ratings yet
- Analysis of Filling System and Consequences of Misfiled Patient Case FoldersDocument23 pagesAnalysis of Filling System and Consequences of Misfiled Patient Case FoldersPelumi Adebayo100% (1)
- Abstract PostDocument1 pageAbstract PostHerry LuanmaseNo ratings yet
- Evaluation and Management of Dysphagia: An Evidence-Based ApproachFrom EverandEvaluation and Management of Dysphagia: An Evidence-Based ApproachDhyanesh A. PatelNo ratings yet
- D882 - Pruebas A Películas.Document11 pagesD882 - Pruebas A Películas.CamiloSilvaNo ratings yet
- COA Full Syllabus-CSEDocument3 pagesCOA Full Syllabus-CSEAMARTYA KUMARNo ratings yet
- Tally QuestionsDocument73 pagesTally QuestionsVishal Shah100% (1)
- Rohini 43569840920Document4 pagesRohini 43569840920SowmyaNo ratings yet
- Efectele Crizei Economice Asupra Politicilor Pietei Muncii Din RomaniaDocument24 pagesEfectele Crizei Economice Asupra Politicilor Pietei Muncii Din Romaniacristian_incaltarauNo ratings yet
- MunnarDocument5 pagesMunnarvisujinuNo ratings yet
- Frito LaysDocument6 pagesFrito LaysElcamino Torrez50% (2)
- What is Software Development Life Cycle (SDLC)? Key Phases and ActivitiesDocument11 pagesWhat is Software Development Life Cycle (SDLC)? Key Phases and ActivitiessachinNo ratings yet
- 15 04 06 SCDocument30 pages15 04 06 SCSugarNo ratings yet
- 0 - Theories of MotivationDocument5 pages0 - Theories of Motivationswathi krishnaNo ratings yet
- Oracle Weblogic Server 12c Administration II - Activity Guide PDFDocument188 pagesOracle Weblogic Server 12c Administration II - Activity Guide PDFNestor Torres Pacheco100% (1)
- PC-II Taftan Master PlanDocument15 pagesPC-II Taftan Master PlanMunir HussainNo ratings yet
- CPWD Contractor Enlistment Rules 2005 SummaryDocument71 pagesCPWD Contractor Enlistment Rules 2005 Summaryvikky717No ratings yet
- Caterpillar Cat 330L EXCAVATOR (Prefix 8FK) Service Repair Manual (8FK00001 and Up)Document27 pagesCaterpillar Cat 330L EXCAVATOR (Prefix 8FK) Service Repair Manual (8FK00001 and Up)kfm8seuuduNo ratings yet
- Bode PlotDocument6 pagesBode PlotChandan S KNo ratings yet
- In Gov cbse-SSCER-191298202020 PDFDocument1 pageIn Gov cbse-SSCER-191298202020 PDFrishichauhan25No ratings yet
- JIG LFO Pack 231 PDFDocument16 pagesJIG LFO Pack 231 PDFPratiek RaulNo ratings yet
- A DETAILED LESSON PLAN IN TLE DraftingDocument16 pagesA DETAILED LESSON PLAN IN TLE DraftingJude PellerinNo ratings yet
- Banking Finance Agile TestingDocument4 pagesBanking Finance Agile Testinganil1karnatiNo ratings yet
- MS For The Access Control System Installation and TerminationDocument21 pagesMS For The Access Control System Installation and Terminationwaaji snapNo ratings yet
- Project Report "A Study of Value Added Tax" "Kirloskar Oil Engines Limited" (Kirloskar Valve Plant)Document4 pagesProject Report "A Study of Value Added Tax" "Kirloskar Oil Engines Limited" (Kirloskar Valve Plant)Sohel BangiNo ratings yet
- Introduction to Soil Investigation ReportDocument76 pagesIntroduction to Soil Investigation ReportRuzengulalebih ZEta's-Listik50% (2)
- A Study of Arcing Fault in The Low-Voltage Electrical InstallationDocument11 pagesA Study of Arcing Fault in The Low-Voltage Electrical Installationaddin100% (1)
- DLL Tle 6 Ict Entrepreneurship 6Document32 pagesDLL Tle 6 Ict Entrepreneurship 6Jewels Garcia100% (1)
- Sys Admin Guide Xerox WorkCentre 7775Document185 pagesSys Admin Guide Xerox WorkCentre 7775dankorzon1No ratings yet
- Lesson 3 - Subtract Two 4-Digit Numbers - More Than One Exchange 2019Document2 pagesLesson 3 - Subtract Two 4-Digit Numbers - More Than One Exchange 2019mNo ratings yet
- Communication Box Specification V1.0Document3 pagesCommunication Box Specification V1.0Natan VillalonNo ratings yet
- Affidavit To Use Surname of The Father - MarquezDocument2 pagesAffidavit To Use Surname of The Father - MarquezReyjohn LodiasNo ratings yet
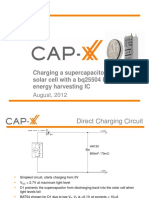
- 1208 CAP XX Charging A Supercapacitor From A Solar Cell PDFDocument12 pages1208 CAP XX Charging A Supercapacitor From A Solar Cell PDFmehralsmenschNo ratings yet
- Introduction To Management: Planning & Goal SettingDocument31 pagesIntroduction To Management: Planning & Goal SettingMaisarah NorzihanNo ratings yet