You might also like
- Heart Dysrhythmias Cheat Sheet PDFDocument5 pagesHeart Dysrhythmias Cheat Sheet PDFbarbaraNo ratings yet
- Common Drug Stems Cheat SheetDocument2 pagesCommon Drug Stems Cheat SheetCharis Mae DimaculanganNo ratings yet
- IV GaugesDocument1 pageIV Gaugesjustin_saneNo ratings yet
- Review The Acute Respiratory Management of Cervical Spinal Cord Injury in The First 6 Weeks After Injury: A Systematic ReviewDocument14 pagesReview The Acute Respiratory Management of Cervical Spinal Cord Injury in The First 6 Weeks After Injury: A Systematic Reviewjustin_saneNo ratings yet
- DM NephroDocument4 pagesDM Nephrojustin_saneNo ratings yet
- Injection Site Cheat Sheet PDFDocument2 pagesInjection Site Cheat Sheet PDFjustin_sane100% (2)
- Cranial Nerves FormDocument2 pagesCranial Nerves FormbarbaraNo ratings yet
- LISDocument7 pagesLISjustin_saneNo ratings yet
- Insulin Cheat SheetDocument1 pageInsulin Cheat Sheetjustin_saneNo ratings yet
- 2004 ConceptsDocument19 pages2004 Conceptsjustin_saneNo ratings yet
- 2012 English Language TestsDocument1 page2012 English Language Testsjustin_saneNo ratings yet
- Applications of Telecounselling in Spinal Cord Injury Rehabilitation: A Systematic Review With Effect SizesDocument13 pagesApplications of Telecounselling in Spinal Cord Injury Rehabilitation: A Systematic Review With Effect Sizesjustin_saneNo ratings yet
- Improving Postoperative Pain Management What Are.40Document6 pagesImproving Postoperative Pain Management What Are.40Luz Adriana Flores PalafoxNo ratings yet
- PDFDocument17 pagesPDFOkri PernandoNo ratings yet
- Applications of Telecounselling in Spinal Cord Injury Rehabilitation: A Systematic Review With Effect SizesDocument13 pagesApplications of Telecounselling in Spinal Cord Injury Rehabilitation: A Systematic Review With Effect Sizesjustin_saneNo ratings yet
- Assessment Nursing Diagnosis Scientific Explanation Planning Interventions Rationale EvaluationDocument2 pagesAssessment Nursing Diagnosis Scientific Explanation Planning Interventions Rationale Evaluationjustin_saneNo ratings yet
- Peptic UlcerrDocument3 pagesPeptic Ulcerrjustin_saneNo ratings yet
- AssessmentDocument10 pagesAssessmentjustin_saneNo ratings yet
- HieDocument24 pagesHiejustin_saneNo ratings yet
- PostOp IlleusDocument8 pagesPostOp Illeusjustin_saneNo ratings yet
- DiagnosticDocument5 pagesDiagnosticjustin_saneNo ratings yet
- DM NephroDocument4 pagesDM Nephrojustin_saneNo ratings yet
- Microsoft Word - Pneumonia Education EnglishDocument9 pagesMicrosoft Word - Pneumonia Education Englishjustin_saneNo ratings yet
- Risk For Infection Pneumonia Nursing Care PlanDocument1 pageRisk For Infection Pneumonia Nursing Care Planjustin_sane100% (1)
- Jurnal HipertensiDocument17 pagesJurnal HipertensiWiny Ch'amhada TtarudaNo ratings yet
- Hyperthermia Pneumonia Nursing Care PlanDocument1 pageHyperthermia Pneumonia Nursing Care Planjustin_saneNo ratings yet
- UlcerDocument24 pagesUlcerjustin_saneNo ratings yet
- DMDocument10 pagesDMjustin_saneNo ratings yet
- 2 Acute Pain Chronic Renal Failure Nursing Care PlansDocument5 pages2 Acute Pain Chronic Renal Failure Nursing Care Plansjustin_saneNo ratings yet
- Physical AssessmentDocument29 pagesPhysical Assessmentjustin_saneNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- MARCOS MUSEUM AND MAUSOLEUMDocument16 pagesMARCOS MUSEUM AND MAUSOLEUMWindel LeoninNo ratings yet
- Open Media Library User ManualDocument60 pagesOpen Media Library User ManualtreelootNo ratings yet
- jQuery Tutorial: Everything You Need to Know About the Popular JavaScript LibraryDocument24 pagesjQuery Tutorial: Everything You Need to Know About the Popular JavaScript LibraryMadhvi JainNo ratings yet
- Academy Architecture and Architectural Review Vol 34 1908Document179 pagesAcademy Architecture and Architectural Review Vol 34 1908q3rNo ratings yet
- Apresiasi Seni Rupa Tiga Dimensi (Seni Patung) FinalDocument67 pagesApresiasi Seni Rupa Tiga Dimensi (Seni Patung) Finalme n sunghoonNo ratings yet
- Sanskrit Librarian Comes AmericaDocument200 pagesSanskrit Librarian Comes AmericaMarinaMariaNo ratings yet
- William Heckscher RembrandtDocument304 pagesWilliam Heckscher RembrandtHortencia AbreuNo ratings yet
- The Complete Works of Lord ByronDocument1,153 pagesThe Complete Works of Lord ByronTovya GibsonNo ratings yet
- Description of STM32F4xx HAL Drivers PDFDocument964 pagesDescription of STM32F4xx HAL Drivers PDFmehmet100% (1)
- Candela Obscura Module - Lost in DreamsDocument9 pagesCandela Obscura Module - Lost in DreamsdasdivyayanNo ratings yet
- GridWorld Case Study ExplainedDocument5 pagesGridWorld Case Study Explainedmdoshi412No ratings yet
- MG0215Document12 pagesMG0215elauwitNo ratings yet
- Management OF Information System: LLLLLLDocument41 pagesManagement OF Information System: LLLLLLThu Hai Le100% (2)
- Practice Test Phonetics and GrammarDocument9 pagesPractice Test Phonetics and GrammarNguyen ThanhNo ratings yet
- Europe ItineraryDocument10 pagesEurope ItineraryRyanNo ratings yet
- Sumerian Texts From The Archive of The Princess Satestar in The Collections of The Iraq MuseumDocument20 pagesSumerian Texts From The Archive of The Princess Satestar in The Collections of The Iraq Museumthanos100% (1)
- Kuc Zylinska - 2016 - Photomediations A Reader PDFDocument321 pagesKuc Zylinska - 2016 - Photomediations A Reader PDFElinoreDarziNo ratings yet
- The Marginal Man Hans Morgenthau PDFDocument286 pagesThe Marginal Man Hans Morgenthau PDFlilianaNo ratings yet
- Odilon Redon (Art Painting Ebook) PDFDocument104 pagesOdilon Redon (Art Painting Ebook) PDFPierrot le Fou100% (2)
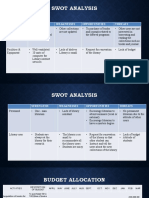
- Swot Analysis: Strengths Weaknesses Opportunities ThreatsDocument3 pagesSwot Analysis: Strengths Weaknesses Opportunities ThreatsIvy JordanNo ratings yet
- Indian Institute of Technology Guwahati: There Are No Dues Against The StudentDocument2 pagesIndian Institute of Technology Guwahati: There Are No Dues Against The StudentAnonymous 8fDg4nNo ratings yet
- C CompilerDocument603 pagesC CompilerpablogadNo ratings yet
- Santiago Calatrava BIODocument3 pagesSantiago Calatrava BIOFiona QuNo ratings yet
- We Are All Made of Molecules by Susin NielsenDocument27 pagesWe Are All Made of Molecules by Susin NielsenRandom House Teens31% (52)
- Stario Csharp SDK Readme v210Document35 pagesStario Csharp SDK Readme v210Bernardo CoutinhoNo ratings yet
- Sadowski 2000 The Sound As An Echo To The Sense: The Iconicity of English GL - WordsDocument66 pagesSadowski 2000 The Sound As An Echo To The Sense: The Iconicity of English GL - WordspotioncomicNo ratings yet
- Skype API GuideDocument62 pagesSkype API Guidesumit8510No ratings yet
- The Great & Beautiful Lost KingdomsDocument11 pagesThe Great & Beautiful Lost KingdomsShabbir Ahmed ChishtiNo ratings yet
- Cbrniac Newsletter Vol14 - Num3Document12 pagesCbrniac Newsletter Vol14 - Num3lzljbNo ratings yet
- Oliver Strunk, Kenneth Levy (Foreword) - Essays On Music in The Byzantine World-W. W. Norton & Company (1977) PDFDocument384 pagesOliver Strunk, Kenneth Levy (Foreword) - Essays On Music in The Byzantine World-W. W. Norton & Company (1977) PDFDimitrios Theodosiou100% (2)