You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Medication Administration GuideDocument204 pagesMedication Administration GuidesaheedvkNo ratings yet
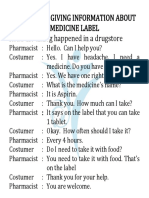
- 3.3 Medicine LabelDocument6 pages3.3 Medicine LabelStefmi Dhila WandaNo ratings yet
- Vicodin Drug Study Que Fransis A.Document3 pagesVicodin Drug Study Que Fransis A.Irene Grace BalcuevaNo ratings yet
- SercDocument3 pagesSerc去約翰100% (1)
- Pharmacy ActDocument32 pagesPharmacy ActAditya Varshneya100% (1)
- Frequently Asked Questions About The Nature of Drug AbuseDocument11 pagesFrequently Asked Questions About The Nature of Drug AbuseKharylle RuñezNo ratings yet
- (Medicinal Chemistry 3) 6sem Questions Bank (B Pharmacy)Document5 pages(Medicinal Chemistry 3) 6sem Questions Bank (B Pharmacy)Someone You knowNo ratings yet
- What Are Drug Utilization Reviews (Dur) : Why Durs Are ImportantDocument3 pagesWhat Are Drug Utilization Reviews (Dur) : Why Durs Are ImportantthegroovyNo ratings yet
- Pedia Tickler 3Document24 pagesPedia Tickler 3Jane GarciaNo ratings yet
- Pantoloc: Uses, Dosing, and Side Effects of the Proton Pump Inhibitor PantoprazoleDocument13 pagesPantoloc: Uses, Dosing, and Side Effects of the Proton Pump Inhibitor PantoprazoleQls LabidezNo ratings yet
- Russian Pharma Market Reaches $1.15 Trillion in 2014Document76 pagesRussian Pharma Market Reaches $1.15 Trillion in 2014Kushal TiwariNo ratings yet
- Pharma Cutoff GenDocument7 pagesPharma Cutoff Gennaitik S TNo ratings yet
- BCS and BDDCS: Classifying Drugs by Solubility, Permeability and MetabolismDocument44 pagesBCS and BDDCS: Classifying Drugs by Solubility, Permeability and MetabolismSiri KalyanNo ratings yet
- Klasifikasi ADRDocument3 pagesKlasifikasi ADRAstari PuspaningdyahNo ratings yet
- Drugs Used To Reduce Gastric Acid SecretionDocument8 pagesDrugs Used To Reduce Gastric Acid Secretiongugus aminaNo ratings yet
- DrugDocument15 pagesDrugknxdg86vk2No ratings yet
- Norpill: Levonorgestrel 1.5 MGDocument1 pageNorpill: Levonorgestrel 1.5 MGShad RahmanNo ratings yet
- List Obat Untuk BidanDocument4 pagesList Obat Untuk BidanlelyNo ratings yet
- Jubilant Life Sciences Receives ANDA Approval For Levetiracetam Injection USP (Company Update)Document2 pagesJubilant Life Sciences Receives ANDA Approval For Levetiracetam Injection USP (Company Update)Shyam SunderNo ratings yet
- MI - ILLINOIS Intraosseous NeedleDocument2 pagesMI - ILLINOIS Intraosseous NeedleFarbodNo ratings yet
- Explain The Importance of Medication Safety Concerning Nursing PracticeDocument4 pagesExplain The Importance of Medication Safety Concerning Nursing Practicechinthaka18389021No ratings yet
- LorazepamDocument4 pagesLorazepamapi-3797941No ratings yet
- Displec m1 SummaryDocument10 pagesDisplec m1 SummaryRafaelaNo ratings yet
- Side Effects of Expare.Document6 pagesSide Effects of Expare.Emelda LaraNo ratings yet
- Antipsychotic Polypharmacy in Clozapine Resistent SchizophreniaDocument24 pagesAntipsychotic Polypharmacy in Clozapine Resistent SchizophreniaI Putu DiatmikaNo ratings yet
- 0907 MigraineheadachesDocument2 pages0907 Migraineheadachesrena_psNo ratings yet
- Wilson & Gisvold's Textbook of Organic Medicinal and Pharmaceutical Chemistry 11th EdDocument1,000 pagesWilson & Gisvold's Textbook of Organic Medicinal and Pharmaceutical Chemistry 11th Edhatipeja76% (33)
- EscitalopramDocument21 pagesEscitalopramalejandra torresNo ratings yet
- 07 Lamp. VII ALAT KESEHATAN 2 PDFDocument19 pages07 Lamp. VII ALAT KESEHATAN 2 PDFDinan Bagja NugrahaNo ratings yet
- Pharmacology Questions With AnswersDocument84 pagesPharmacology Questions With AnswersAquiles Vaesto100% (9)