You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- I68regenerator Language TemplateDocument2 pagesI68regenerator Language TemplateSebastian AlecuNo ratings yet
- Correlations: Kuisioner Sindroma DispepsiaDocument2 pagesCorrelations: Kuisioner Sindroma DispepsiaDimas AgungNo ratings yet
- Daftar PustakaDocument1 pageDaftar PustakaDimas AgungNo ratings yet
- Daftar Singkatan BTA Bakteri Tahan Asam TB Tuberculosis WHO World Health Organization Puskesmas Pusat Kesehatan Masyarakat PMO Pengawas Minum ObatDocument1 pageDaftar Singkatan BTA Bakteri Tahan Asam TB Tuberculosis WHO World Health Organization Puskesmas Pusat Kesehatan Masyarakat PMO Pengawas Minum ObatDimas AgungNo ratings yet
- Kuisioner Sindroma Dispepsia dan Pola MakanDocument3 pagesKuisioner Sindroma Dispepsia dan Pola MakanDimas AgungNo ratings yet
- Patient Complaint DataDocument13 pagesPatient Complaint DataDimas AgungNo ratings yet
- Daftar Pustaka PksDocument1 pageDaftar Pustaka PksDimas AgungNo ratings yet
- Abstract Dimas FK UnjaDocument2 pagesAbstract Dimas FK UnjaDimas AgungNo ratings yet
- Abstract Dimas FK UnjaDocument2 pagesAbstract Dimas FK UnjaDimas AgungNo ratings yet
- Wish You Were Here (Hey Monday)Document1 pageWish You Were Here (Hey Monday)Dimas AgungNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Scientific DrawningsDocument6 pagesScientific Drawningsichbinangus100% (1)
- Leslie Pray, Ph.D. 2008. Recombinant DNA Technology and Transgenic AnimalsDocument5 pagesLeslie Pray, Ph.D. 2008. Recombinant DNA Technology and Transgenic AnimalsJosé Jhair Enrique IIINo ratings yet
- Genes Hearing DeafnessDocument328 pagesGenes Hearing DeafnessjvojnicNo ratings yet
- Natural Science 3Document3 pagesNatural Science 3Nika LD100% (1)
- Cushnie and Lamb (2005)Document16 pagesCushnie and Lamb (2005)ayu alfiantiNo ratings yet
- Gregor Mendel NotesDocument2 pagesGregor Mendel NotesAleczander EstrebilloNo ratings yet
- Anthropology Syllabus (Paper 1) : S.no Syllabus Reference BooksDocument6 pagesAnthropology Syllabus (Paper 1) : S.no Syllabus Reference BooksBhaskar NNo ratings yet
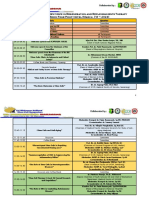
- Susunan Acara SimposiumDocument5 pagesSusunan Acara SimposiumRisal FoengNo ratings yet
- Tutorial RDocument456 pagesTutorial RCrystal GranadosNo ratings yet
- Exercise 5 Molecular Basis of HeredityDocument6 pagesExercise 5 Molecular Basis of HeredityHiroshi MatsushimaNo ratings yet
- Evoulution and GeneticsDocument5 pagesEvoulution and GeneticsASUPREMEANo ratings yet
- Mitosis Quiz 17 04 2015Document6 pagesMitosis Quiz 17 04 2015api-296545639100% (1)
- 1.study of Physiological Functions of Digestive System of Farm AnimalsDocument58 pages1.study of Physiological Functions of Digestive System of Farm AnimalsKashifNo ratings yet
- Lec 10 AntiviralsDocument26 pagesLec 10 AntiviralsAiqa QaziNo ratings yet
- Biology Project Pedigree Analysis Class 12Document28 pagesBiology Project Pedigree Analysis Class 12PrateekBansal61% (36)
- NR 23 Strictly Anaerobic Beer Spoilage Bacteria With Special Emphasis On New and Emerging Species Riikka JuvonenDocument37 pagesNR 23 Strictly Anaerobic Beer Spoilage Bacteria With Special Emphasis On New and Emerging Species Riikka JuvonenIvana NikolicNo ratings yet
- 21 Pathogenesis of Carp Erythrodermatitis (CE)Document6 pages21 Pathogenesis of Carp Erythrodermatitis (CE)giuseppegnrNo ratings yet
- Utility of The Sputum Cytology Applying MGG and Pap Stains in Monitoring Sudanese Patients Complaining of Bronchial AsthmaDocument6 pagesUtility of The Sputum Cytology Applying MGG and Pap Stains in Monitoring Sudanese Patients Complaining of Bronchial AsthmaDr. Asaad Mohammed Ahmed BabkerNo ratings yet
- WikiPharma Database Provides Ecotoxicity DataDocument5 pagesWikiPharma Database Provides Ecotoxicity DataRaluca RatiuNo ratings yet
- Nac Change Letter FinalDocument6 pagesNac Change Letter Finalapi-319146946No ratings yet
- Regulation of Gene ExpressionDocument1 pageRegulation of Gene ExpressionhomamunfatNo ratings yet
- Platelet-Rich Plasma (PRP) : What Is PRP and What Is Not PRP?Document4 pagesPlatelet-Rich Plasma (PRP) : What Is PRP and What Is Not PRP?Amanda PutriNo ratings yet
- Alfalfa GrowthDocument22 pagesAlfalfa GrowthEkaterina BogatyrevaNo ratings yet
- N20 H2 P2 Answers-1Document10 pagesN20 H2 P2 Answers-1Samuel TeohNo ratings yet
- SCIENCE Grade 7: Quarter 2 - Module 3 Cell To BiosphereDocument12 pagesSCIENCE Grade 7: Quarter 2 - Module 3 Cell To BiosphereMarie Pearl F. Adamos100% (1)
- Ecosystem Structure and Types EcosystemDocument27 pagesEcosystem Structure and Types EcosystemMOVIES starNo ratings yet
- A tree is a producer. Bacteria can be decomposers. An eagle is a secondary consumerDocument37 pagesA tree is a producer. Bacteria can be decomposers. An eagle is a secondary consumerScience,Physical Education And Sports VideosNo ratings yet
- Prelim Quizzes With AnswerDocument9 pagesPrelim Quizzes With AnswerNAOMI BATAYOLANo ratings yet
- Aerobic and Anaerobic Pathways - An Introduction To The Energy SystemsDocument33 pagesAerobic and Anaerobic Pathways - An Introduction To The Energy SystemsMary Grace Dela PeñaNo ratings yet
- Cellular ReproductionDocument48 pagesCellular ReproductionOttah Simon UdochiNo ratings yet