You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- CV Clinical Coordinator Resume Highlights Phase III Trials ExperienceDocument3 pagesCV Clinical Coordinator Resume Highlights Phase III Trials ExperiencepranatiprustyNo ratings yet
- Pusat Bahasa UNAIR - Portal - 13 Maret Jam 13Document1 pagePusat Bahasa UNAIR - Portal - 13 Maret Jam 13dr. M.F. RomdhoniNo ratings yet
- Bod DiabetesDocument28 pagesBod Diabetesdr. M.F. RomdhoniNo ratings yet
- Type 2 Diabetes MellitusDocument24 pagesType 2 Diabetes Mellitusdr. M.F. Romdhoni100% (1)
- Antinociceptive and Edematogenic Activity and Chemical ConstituentsDocument10 pagesAntinociceptive and Edematogenic Activity and Chemical Constituentsdr. M.F. RomdhoniNo ratings yet
- Bod DiabetesDocument28 pagesBod Diabetesdr. M.F. RomdhoniNo ratings yet
- 29 EMDAC B1 03 Guest CoreSlidesDocument186 pages29 EMDAC B1 03 Guest CoreSlidesdr. M.F. RomdhoniNo ratings yet
- Cme DMT2 PDFDocument77 pagesCme DMT2 PDFdr. M.F. RomdhoniNo ratings yet
- ParacetamolDocument13 pagesParacetamolSusi Ferawati100% (1)
- Investigational New Drug Application (IND)Document48 pagesInvestigational New Drug Application (IND)Divya100% (1)
- Basic Principles of Pharmacology Handout PDFDocument111 pagesBasic Principles of Pharmacology Handout PDFRazel Kinette AzotesNo ratings yet
- Natural Products in Drug DiscoveryDocument8 pagesNatural Products in Drug DiscoveryartemisinNo ratings yet
- Week 1 Introduction To PharmacologyDocument12 pagesWeek 1 Introduction To PharmacologyDino MicaNo ratings yet
- Current Scenario of Biologics in IndiaDocument30 pagesCurrent Scenario of Biologics in IndiaShivang Shah100% (1)
- Endotoxin Limits For Parenteral Drug Products: by Mick DawsonDocument7 pagesEndotoxin Limits For Parenteral Drug Products: by Mick DawsonEduardo LozanoNo ratings yet
- HTTPS://WWW - Scribd.com/document/434187554/compendium of Therapeutic Choices Canadas Trusted Reference For Primary Care Therapeutics CTC 7 Book PDFDocument19 pagesHTTPS://WWW - Scribd.com/document/434187554/compendium of Therapeutic Choices Canadas Trusted Reference For Primary Care Therapeutics CTC 7 Book PDFShanaya ShergillNo ratings yet
- PK-Factors Prolonging Drug Action-1Document18 pagesPK-Factors Prolonging Drug Action-1Manikanta GupthaNo ratings yet
- Walgreen Online PharmacyDocument64 pagesWalgreen Online PharmacyWalgreen Online PharmacyNo ratings yet
- Recommendation of SEC (Oncology) Dated 10.03.2021 & 11.03.2021Document6 pagesRecommendation of SEC (Oncology) Dated 10.03.2021 & 11.03.2021rx bafnaNo ratings yet
- Daftar Lasa N High Alert PKM SambasDocument5 pagesDaftar Lasa N High Alert PKM SambasROBERTNo ratings yet
- Pharmaceutical Dosage Forms, Drug Delivery Systems and Medical Devices Pharm 201L Name:Tallod, Emerson John L. Group:11 Year/Section:Q2A Final RatingDocument7 pagesPharmaceutical Dosage Forms, Drug Delivery Systems and Medical Devices Pharm 201L Name:Tallod, Emerson John L. Group:11 Year/Section:Q2A Final RatingJames AzurinNo ratings yet
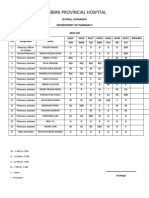
- Lumbini Hospital Pharmacy Duty RosterDocument2 pagesLumbini Hospital Pharmacy Duty RosterImdadHussainOPositiveNo ratings yet
- Weekly Sales Performance and Product Promotion ReportDocument6 pagesWeekly Sales Performance and Product Promotion ReportZelalemNo ratings yet
- Pavitt 2000 - Academic Research in EuropeDocument15 pagesPavitt 2000 - Academic Research in Europeapi-27028656No ratings yet
- Enzyme Crossword: Key Terms for Enzyme ActivityDocument3 pagesEnzyme Crossword: Key Terms for Enzyme ActivityormattNo ratings yet
- RSUP SanglahDocument42 pagesRSUP Sanglahgexcha_kazoebNo ratings yet
- VP Health Biomedical Research in Washington DC Resume Richard HaberbergerDocument3 pagesVP Health Biomedical Research in Washington DC Resume Richard HaberbergerRichardHaberbergerNo ratings yet
- Assessment of Prospective & Inactive AccountsDocument29 pagesAssessment of Prospective & Inactive AccountsHazel BandayNo ratings yet
- Test Bank For Drug Use and Abuse 8th EditionDocument36 pagesTest Bank For Drug Use and Abuse 8th Editionoverspanchitter4abo100% (37)
- Clinical PharmacyDocument7 pagesClinical PharmacyKabir ManchandaNo ratings yet
- Ra 10918 BsaDocument19 pagesRa 10918 BsarimNo ratings yet
- Kendala UTS Online Genap 2019-2020 (Responses)Document77 pagesKendala UTS Online Genap 2019-2020 (Responses)Rahma Fauzia MadhaningrumNo ratings yet
- List of Pharmaceutical Manufacturer in BangladeshDocument11 pagesList of Pharmaceutical Manufacturer in Bangladeshsujal0211100% (1)
- Basic Principles of PharmacologyDocument47 pagesBasic Principles of Pharmacologysapiah raman100% (2)
- 2005 Pha5127 Final PDFDocument17 pages2005 Pha5127 Final PDFBaguma MichaelNo ratings yet
- PHC 401 Sept 2015Document8 pagesPHC 401 Sept 2015RedzaHanifNo ratings yet