You might also like
- P8 Carrivick - Anti-Mullerian Hormone Stability - Effects of Temperature and TimeDocument1 pageP8 Carrivick - Anti-Mullerian Hormone Stability - Effects of Temperature and TimeYondri Mandaku TasidjawaNo ratings yet
- Protein Metabolism: Department of Biochemistry Medical Faculti of Hasanuddin UniversityDocument80 pagesProtein Metabolism: Department of Biochemistry Medical Faculti of Hasanuddin UniversityYondri Mandaku TasidjawaNo ratings yet
- Cell Base Model of HaemostasisDocument25 pagesCell Base Model of HaemostasisYondri Mandaku TasidjawaNo ratings yet
- Circulating Fragments of N-Terminal Pro-B-Type Natriuretic Peptides in Plasma of Heart Failure PatientsDocument9 pagesCirculating Fragments of N-Terminal Pro-B-Type Natriuretic Peptides in Plasma of Heart Failure PatientsYondri Mandaku TasidjawaNo ratings yet
- Red Wine and Diabetes Health: Getting Skin in The Game: R. Paul RobertsonDocument8 pagesRed Wine and Diabetes Health: Getting Skin in The Game: R. Paul RobertsonYondri Mandaku TasidjawaNo ratings yet
- Pato Fisiologi Kuliah 4 TemperatureDocument16 pagesPato Fisiologi Kuliah 4 TemperatureYondri Mandaku TasidjawaNo ratings yet
- Detection IHCDocument129 pagesDetection IHCYondri Mandaku TasidjawaNo ratings yet
- Haider Study (2 PerhidrosisDocument7 pagesHaider Study (2 PerhidrosisYondri Mandaku TasidjawaNo ratings yet
- Blood Bank Lab WorksheetDocument1 pageBlood Bank Lab WorksheetYondri Mandaku TasidjawaNo ratings yet
- Urin 1Document10 pagesUrin 1Mardatillah WiranataNo ratings yet
- Bio Identical VitaminsDocument24 pagesBio Identical VitaminshamzaloNo ratings yet
- All About AnorexiaDocument19 pagesAll About Anorexiajdthx4uNo ratings yet
- Nutrients 04 00208 v2Document23 pagesNutrients 04 00208 v2Yondri Mandaku TasidjawaNo ratings yet
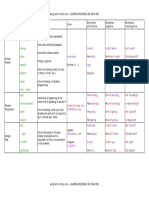
- Tenses Table PDFDocument5 pagesTenses Table PDFAlejandra Neira GonzálezNo ratings yet
- Laparoscopic Sleeve Gastrectomy: Perioperative Outcomes, Weight Loss and Impact On Type 2 Diabetes Mellitus Over 2 YearsDocument5 pagesLaparoscopic Sleeve Gastrectomy: Perioperative Outcomes, Weight Loss and Impact On Type 2 Diabetes Mellitus Over 2 YearsYondri Mandaku TasidjawaNo ratings yet
- Curva ROC Metabolk-PasienDocument1 pageCurva ROC Metabolk-PasienYondri Mandaku TasidjawaNo ratings yet
- Artigo 13 - DM GestacionalDocument8 pagesArtigo 13 - DM GestacionalfahlevyNo ratings yet
- Critical Evaluation of Diagnosis and Outcomes of Gestational DiabetesDocument23 pagesCritical Evaluation of Diagnosis and Outcomes of Gestational DiabetesYondri Mandaku TasidjawaNo ratings yet
- 2147 FullDocument8 pages2147 FullYondri Mandaku TasidjawaNo ratings yet
- Print 1Document11 pagesPrint 1Yondri Mandaku TasidjawaNo ratings yet
- Nutrients: The Potential Role of Vitamin D Enhanced Foods in Improving Vitamin D StatusDocument19 pagesNutrients: The Potential Role of Vitamin D Enhanced Foods in Improving Vitamin D StatusYondri Mandaku TasidjawaNo ratings yet
- ADA Standards of Medical Care 2013 FINAL 21 Dec 2012Document146 pagesADA Standards of Medical Care 2013 FINAL 21 Dec 2012Mike MythiasNo ratings yet
- 260 FullDocument7 pages260 FullYondri Mandaku TasidjawaNo ratings yet
- Healing Power of Sunlight and Witamin DDocument26 pagesHealing Power of Sunlight and Witamin Djecan100% (1)
- D-Vitamin PLOS OneDocument7 pagesD-Vitamin PLOS OneYondri Mandaku TasidjawaNo ratings yet
- Aus Anorexia Nervosa PDFDocument31 pagesAus Anorexia Nervosa PDFYondri Mandaku Tasidjawa100% (1)
- Ijo 201233 ADocument8 pagesIjo 201233 AYondri Mandaku TasidjawaNo ratings yet
- Duvvuri2009AnorexiaNervosa PDFDocument8 pagesDuvvuri2009AnorexiaNervosa PDFYondri Mandaku TasidjawaNo ratings yet
- GDM PresetationDocument26 pagesGDM PresetationYondri Mandaku TasidjawaNo ratings yet
- Aus Anorexia Nervosa PDFDocument31 pagesAus Anorexia Nervosa PDFYondri Mandaku Tasidjawa100% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Case Analysis OBDocument10 pagesCase Analysis OBRuchita Munish33% (3)
- Odisha Child ProtectionDocument7 pagesOdisha Child Protectionvishesh anandNo ratings yet
- BES-121 Childhood and Growing UpDocument57 pagesBES-121 Childhood and Growing UpPulkesh PulakNo ratings yet
- Understanding SociologyDocument11 pagesUnderstanding SociologyheretostudyNo ratings yet
- Educ 101 Module 1Document12 pagesEduc 101 Module 1Kyle GomezNo ratings yet
- Dichotomy of Masochism Without SadismDocument18 pagesDichotomy of Masochism Without SadismLaura SfarghiuNo ratings yet
- Nickelodeon #KidsTogether Guide: Talking With Kids About CoronavirusDocument2 pagesNickelodeon #KidsTogether Guide: Talking With Kids About CoronavirusDerek E. BairdNo ratings yet
- TRAINING AND DEVELOPMENT SURVEYDocument32 pagesTRAINING AND DEVELOPMENT SURVEYKhushboo KhannaNo ratings yet
- British Airways Recruitment StrategyDocument2 pagesBritish Airways Recruitment StrategyAbhishek Srivastava100% (1)
- How People Navigate Urban EnvironmentsDocument4 pagesHow People Navigate Urban EnvironmentsJames AsasNo ratings yet
- A Project Manager's OptimismDocument18 pagesA Project Manager's OptimismIna NafaNo ratings yet
- GL Bajaj FormateDocument5 pagesGL Bajaj FormateFARMANNo ratings yet
- SENG James T. Webb Scholarship Application: Family Information FormDocument4 pagesSENG James T. Webb Scholarship Application: Family Information FormAnonymous gjKuCDONo ratings yet
- Reading and Writing 3 Q: Skills For Success Unit 6 Student Book Answer KeyDocument3 pagesReading and Writing 3 Q: Skills For Success Unit 6 Student Book Answer Keybichhanh142No ratings yet
- Akashic Record - Edgar Caycee Readings (Reporting Transcript)Document8 pagesAkashic Record - Edgar Caycee Readings (Reporting Transcript)School Desk SpaceNo ratings yet
- The Intersection of History, Literature and Trauma in Chimamanda Ngozi Adichie's HalfDocument60 pagesThe Intersection of History, Literature and Trauma in Chimamanda Ngozi Adichie's HalfHouda BoursNo ratings yet
- Full Download Test Bank For Cultural Psychology 4th Edition Steven J Heine PDF Full ChapterDocument36 pagesFull Download Test Bank For Cultural Psychology 4th Edition Steven J Heine PDF Full Chaptermolecast.bassawkzaa100% (15)
- López Cano, Rubén. Musica PoeticaDocument0 pagesLópez Cano, Rubén. Musica PoeticaChacototototeNo ratings yet
- Brand Resonance ModelDocument3 pagesBrand Resonance ModelNaimul KaderNo ratings yet
- De Thi HSG Anh Lop 9 Bang A - Nghe An 2018-2019Document8 pagesDe Thi HSG Anh Lop 9 Bang A - Nghe An 2018-2019Thủy Nguyễn ThịNo ratings yet
- Cultural Traits Can Assume Various Forms Which Have Meanings. The Statement Implies That Culture IsDocument21 pagesCultural Traits Can Assume Various Forms Which Have Meanings. The Statement Implies That Culture IsmercyvienhoNo ratings yet
- A Guide To Endorsed Resources From CambridgeDocument2 pagesA Guide To Endorsed Resources From CambridgesamNo ratings yet
- Kabit and HiyaDocument2 pagesKabit and HiyaEarl Danzell SantosNo ratings yet
- Module 5 SuctioningDocument2 pagesModule 5 SuctioningDcimasaNo ratings yet
- English Grammar Modul Grade 10Document123 pagesEnglish Grammar Modul Grade 10Aaron HartonoNo ratings yet
- Case Study Isales Jan Edzel Isales Elaine JoyDocument9 pagesCase Study Isales Jan Edzel Isales Elaine JoyJan Edzel Batilo IsalesNo ratings yet
- Uts Module 3 The Digital SelfDocument4 pagesUts Module 3 The Digital SelfTinay Ledesma GepetacioNo ratings yet
- Oedipus Rex - Key AssessmentDocument3 pagesOedipus Rex - Key AssessmentIoanna MantaNo ratings yet
- Career Reflection PaperDocument7 pagesCareer Reflection Paperapi-4879323160% (1)
- Utilitarian Ethics in a NutshellDocument20 pagesUtilitarian Ethics in a Nutshelljessabhel bositoNo ratings yet