You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- BasketballDocument19 pagesBasketballDamir SpahićNo ratings yet
- 365 Strong - Lilly PDFDocument69 pages365 Strong - Lilly PDF健身老扈No ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Rts 10 Weeks CycleDocument3 pagesRts 10 Weeks CycleChris VisNo ratings yet
- VolleyballDocument27 pagesVolleyballMaraNo ratings yet
- The History and Rules of Table TennisDocument6 pagesThe History and Rules of Table TennisKaryl Aarientos100% (1)
- Tabloid Activities: 1. Kalq 5. TarnambaiDocument1 pageTabloid Activities: 1. Kalq 5. Tarnambaiapi-396577001No ratings yet
- PE 4 Mod 1 21-22Document25 pagesPE 4 Mod 1 21-22JULLIE CARMELLE H. CHATTONo ratings yet
- AB de Villiers Career, Records, Facts & Net WorthDocument3 pagesAB de Villiers Career, Records, Facts & Net WorthAbhi RamNo ratings yet
- Impact of Various Plyometric Training On Skill Performance in Football PlayersDocument1 pageImpact of Various Plyometric Training On Skill Performance in Football PlayersRajesh WilliamNo ratings yet
- Table TennisDocument14 pagesTable TennisAarush GuptaNo ratings yet
- Titans Lacrosse Official PlaybookDocument18 pagesTitans Lacrosse Official Playbookcoachvint1980No ratings yet
- KUD ChartDocument2 pagesKUD Chartjenny_hamlinNo ratings yet
- Sepep Lesson PlanDocument6 pagesSepep Lesson Planapi-345271242No ratings yet
- FIFA World Cup 2022 Schedule Excel SheetDocument4 pagesFIFA World Cup 2022 Schedule Excel Sheetfeed my mindNo ratings yet
- NFHS Exam Soccer 2017Document17 pagesNFHS Exam Soccer 2017MOEDNo ratings yet
- Lionel Andrés Messi Cuccittini: (Note 1) (A)Document3 pagesLionel Andrés Messi Cuccittini: (Note 1) (A)Rodrigo F OrtegaNo ratings yet
- Path Fit 4 Sports: Volleyball FundamentalsDocument29 pagesPath Fit 4 Sports: Volleyball FundamentalsNina BachoNo ratings yet
- Intramurals 2022Document13 pagesIntramurals 2022ANGIELO PAHAMUTANGNo ratings yet
- Matchdata - Ipynb - ColaboratoryDocument3 pagesMatchdata - Ipynb - Colaboratorybasilnaeem7No ratings yet
- forest city ms boys track info sheet 2024Document3 pagesforest city ms boys track info sheet 2024api-253710069No ratings yet
- Netball Defending SkillsDocument2 pagesNetball Defending SkillsdeeNo ratings yet
- PPL PowerbuildingDocument4 pagesPPL PowerbuildingennesNo ratings yet
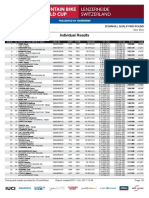
- Lenz Dhi Me Results QRDocument5 pagesLenz Dhi Me Results QRDirt MagazineNo ratings yet
- Measurable SportsDocument10 pagesMeasurable SportsKassy AlcaldezaNo ratings yet
- Ball Badminton Entry FormDocument2 pagesBall Badminton Entry Formvelmurugan_jNo ratings yet
- Federer's Racquets v0.2Document12 pagesFederer's Racquets v0.2Rahul SinghNo ratings yet
- Mr. John SmithGIRLS TOUCH RUGBY Alyssa Chan Jenny Cheng Jenny Chung Jenny FungDocument24 pagesMr. John SmithGIRLS TOUCH RUGBY Alyssa Chan Jenny Cheng Jenny Chung Jenny FungTara MorrisonNo ratings yet
- NBA 2K13 Playbook and SlidersDocument241 pagesNBA 2K13 Playbook and SlidersMinn21tNo ratings yet
- Kabadi IDocument10 pagesKabadi IBishal KhaidemNo ratings yet
- 2012 Brooks PR Invitational Media GuideDocument24 pages2012 Brooks PR Invitational Media GuideBrooksRunningNo ratings yet