You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Postpartum Discharge PlanDocument3 pagesPostpartum Discharge PlanCassey CamamaNo ratings yet
- ICMRDocument12 pagesICMRAnil KumarNo ratings yet
- hf305 00 Dfu DeuDocument54 pageshf305 00 Dfu DeuMauro EzechieleNo ratings yet
- Thesis On Hypertension in PregnancyDocument7 pagesThesis On Hypertension in Pregnancydwt29yrp100% (2)
- Autonomic Dysfunction and Hypotension: Christopher J. MathiasDocument28 pagesAutonomic Dysfunction and Hypotension: Christopher J. MathiaswaltercarvalhoNo ratings yet
- Fi H 0840 004 ParDocument16 pagesFi H 0840 004 ParNathaniel Roi BalbarinoNo ratings yet
- PED 001 Module (Prelim)Document37 pagesPED 001 Module (Prelim)Keith Ian JulianNo ratings yet
- TB4-Frag A Collection of StudiesDocument20 pagesTB4-Frag A Collection of StudiesscribdNo ratings yet
- Management of Chronic Kidney Disease (Mutraghata) Through Ayurveda Regimen: A Case ReportDocument12 pagesManagement of Chronic Kidney Disease (Mutraghata) Through Ayurveda Regimen: A Case ReportakhilkgNo ratings yet
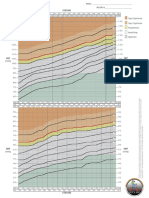
- BP Chart Boys Color WideDocument1 pageBP Chart Boys Color WidealbertNo ratings yet
- Combination of Lisinopril and Nifedipine GITS.10Document7 pagesCombination of Lisinopril and Nifedipine GITS.10Andi PermanaNo ratings yet
- Health and Vastu Shastra Tips For Happy Life - SubhaVaastuDocument14 pagesHealth and Vastu Shastra Tips For Happy Life - SubhaVaastuMadhu46dNo ratings yet
- Management of Acute Ischemic Stroke.13Document10 pagesManagement of Acute Ischemic Stroke.13Juan fernando Torres pavaNo ratings yet
- ACOG Practice Bulletin No 202Document25 pagesACOG Practice Bulletin No 202Berri RahmadhoniNo ratings yet
- Merck Interest AreasDocument40 pagesMerck Interest AreasPhil MurrayNo ratings yet
- EMS Field Handbook (Revision 1) PDFDocument61 pagesEMS Field Handbook (Revision 1) PDFAnonymous qAEhQo1No ratings yet
- Understanding Cardiomyopathies and Cardiac Conduction DisordersDocument86 pagesUnderstanding Cardiomyopathies and Cardiac Conduction DisordersStarr Newman100% (1)
- Dental Care For Patients With Heart Failure: An UpdateDocument9 pagesDental Care For Patients With Heart Failure: An UpdateGustavo A OrtegonNo ratings yet
- Hypertension Topic DiscussionDocument13 pagesHypertension Topic Discussionapi-665372449No ratings yet
- Aprovel TabletDocument7 pagesAprovel Tabletramesh4321No ratings yet
- Diabetes Among HIV-Infected Patients On Antiretroviral Therapy at Mulago National Referral Hospital in Central UgandaDocument6 pagesDiabetes Among HIV-Infected Patients On Antiretroviral Therapy at Mulago National Referral Hospital in Central UgandaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 56 JOE Hypert Peria Cond 2010Document6 pages56 JOE Hypert Peria Cond 2010nurima diyahNo ratings yet
- Jurnal InternationalDocument9 pagesJurnal InternationalRulix SevenfoldNo ratings yet
- User Manual: Blood Pressure Monitor EBP-095 Arm TypeDocument14 pagesUser Manual: Blood Pressure Monitor EBP-095 Arm TypeRhea Jane B. CatalanNo ratings yet
- Ritalin LaDocument20 pagesRitalin Lamichele.siciliano4467No ratings yet
- Chlorthalidone, Not Hydrochlorothiazide, Is The Right Diuretic For ComparisonDocument2 pagesChlorthalidone, Not Hydrochlorothiazide, Is The Right Diuretic For ComparisonZeba Sohel KhatriNo ratings yet
- Serpentina Treatment: A Review of LiteratureDocument11 pagesSerpentina Treatment: A Review of LiteraturedanisterNo ratings yet
- Vegan Soul Food Cookbook Plant-Based, No-Fuss Southern Favorites by Nadira Jenkins-ElDocument209 pagesVegan Soul Food Cookbook Plant-Based, No-Fuss Southern Favorites by Nadira Jenkins-ElRomylar Dee100% (3)
- Textbook Geriatric Psychiatry 09 PDFDocument23 pagesTextbook Geriatric Psychiatry 09 PDFLydia AmaliaNo ratings yet
- Roth 10e Nclex Chapter 11Document4 pagesRoth 10e Nclex Chapter 11jennaaahhhNo ratings yet