You might also like
- Top Secret Programs Hidden in Plain SightDocument296 pagesTop Secret Programs Hidden in Plain SightTee R Taylor100% (5)
- Psych DictDocument238 pagesPsych DictTee R Taylor100% (1)
- ADL Hate On Display PrintableDocument60 pagesADL Hate On Display PrintableTee R TaylorNo ratings yet
- 1917 Trading With The Enemy ActDocument17 pages1917 Trading With The Enemy ActJanus007100% (1)
- 1917 Trading With The Enemy ActDocument17 pages1917 Trading With The Enemy ActJanus007100% (1)
- Black Book of ScamsDocument72 pagesBlack Book of ScamsSolert100% (1)
- Con Men ScamsDocument14 pagesCon Men ScamsTee R TaylorNo ratings yet
- Donchian 4 W PDFDocument33 pagesDonchian 4 W PDFTheodoros Maragakis100% (2)
- Gun Care Guide: Rifle Shotgun Handgun Black PowderDocument17 pagesGun Care Guide: Rifle Shotgun Handgun Black PowderTee R TaylorNo ratings yet
- Problem-Solution Essay Final DraftDocument4 pagesProblem-Solution Essay Final Draftapi-490864786No ratings yet
- A Terence McKenna Audio Archive - Part 1Document203 pagesA Terence McKenna Audio Archive - Part 1BabaYagaNo ratings yet
- The Con Artist's Playbook: The Psychology Behind ID Theft, Fraud & ScamsDocument9 pagesThe Con Artist's Playbook: The Psychology Behind ID Theft, Fraud & ScamsAnshulNo ratings yet
- Commercial LawDocument61 pagesCommercial LawthebfilesNo ratings yet
- Smoking Cessation ProgramDocument5 pagesSmoking Cessation ProgrampeterjongNo ratings yet
- Football Trading StrategyDocument27 pagesFootball Trading StrategyChem100% (2)
- Accredited Hypnosis Hypnotherapy Certification TrainingDocument7 pagesAccredited Hypnosis Hypnotherapy Certification TrainingTee R TaylorNo ratings yet
- Past Simple Present Perfect ExercisesDocument3 pagesPast Simple Present Perfect ExercisesAmanda Trujillo100% (1)
- DLL Ict 9 1st Quarter Week 5Document3 pagesDLL Ict 9 1st Quarter Week 5Bernadeth Irma Sawal Caballa100% (2)
- b-gl-392-003fp-001 - 30 May 2002 RAPPELLING TECHNIQUES AND PROCEDURESDocument75 pagesb-gl-392-003fp-001 - 30 May 2002 RAPPELLING TECHNIQUES AND PROCEDURESTiterNo ratings yet
- People Vs GonaDocument2 pagesPeople Vs GonaM Azeneth JJ100% (1)
- Smoking Cessation: What Good Will Doctor's Advice Do?Document6 pagesSmoking Cessation: What Good Will Doctor's Advice Do?Getstop SmokingNo ratings yet
- Research On Drugs AbuseDocument8 pagesResearch On Drugs AbusefredrickfoleyNo ratings yet
- Chapter-British Parliamentary Debate FormatDocument8 pagesChapter-British Parliamentary Debate FormatNoelle HarrisonNo ratings yet
- Stop Smoking: Proven Steps And Strategies To Make You Quit Smoking For GoodFrom EverandStop Smoking: Proven Steps And Strategies To Make You Quit Smoking For GoodRating: 4 out of 5 stars4/5 (1)
- Tobacco Cessation PlanDocument11 pagesTobacco Cessation PlanEsteban García EcheverryNo ratings yet
- Five Ways To Quit Smoking: Group 3Document5 pagesFive Ways To Quit Smoking: Group 3LuOne NitaNo ratings yet
- CE Winter Smoking CessationDocument7 pagesCE Winter Smoking CessationMiclăuș GeorgeNo ratings yet
- Smoking Cessation Final FileDocument2 pagesSmoking Cessation Final Fileirene lumactodNo ratings yet
- Persuasive LetterDocument7 pagesPersuasive LetterRuby JosephNo ratings yet
- Healthcare Professionals Health Systems HDocument2 pagesHealthcare Professionals Health Systems HARAFAT MIAHNo ratings yet
- Committee Opinion: Tobacco Use and Women'S HealthDocument5 pagesCommittee Opinion: Tobacco Use and Women'S HealthAnonymous Bv8iwuYCHFNo ratings yet
- The SANE Smokefree KitDocument129 pagesThe SANE Smokefree KitSANE AustraliaNo ratings yet
- 4 - Tobacco and Substance UseDocument20 pages4 - Tobacco and Substance UseCoral Srinivasa RamaluNo ratings yet
- Want To Be Hale and Strong Even at 80? Quit Smoking Now and Join The Smoking Cessation Program!Document3 pagesWant To Be Hale and Strong Even at 80? Quit Smoking Now and Join The Smoking Cessation Program!Mariah VivasNo ratings yet
- Review of Related Literature CigarettesDocument7 pagesReview of Related Literature CigarettesAngeline TolentinoNo ratings yet
- PMCH: Awareness of The Serious Consequences of Smoking Cigarettes Among Teenagers Studying in UphsdDocument27 pagesPMCH: Awareness of The Serious Consequences of Smoking Cigarettes Among Teenagers Studying in UphsdNakul SrivastavaNo ratings yet
- Negative Health Impacts of Drinking AlcoholDocument43 pagesNegative Health Impacts of Drinking AlcoholGlen CustodioNo ratings yet
- Prevention of Drug AbuseDocument2 pagesPrevention of Drug AbuseIvana Ariane ClaorNo ratings yet
- Assessment 2 EssayDocument5 pagesAssessment 2 EssayMudassar Gul Bin AshrafNo ratings yet
- Effect of Smoking To TeenagersDocument7 pagesEffect of Smoking To TeenagersSiti Haridah AJNo ratings yet
- Accepted ManuscriptDocument40 pagesAccepted ManuscriptsueffximenaNo ratings yet
- Wala KwnetaDocument11 pagesWala KwnetaJohn Vincent Consul CameroNo ratings yet
- Little Known Questions About Alcohol Use Disorder (Aud) : MedlineplusDocument3 pagesLittle Known Questions About Alcohol Use Disorder (Aud) : Medlineplusmaultaose1No ratings yet
- Example of Research Paper About Illegal DrugsDocument6 pagesExample of Research Paper About Illegal Drugsfvhwd4yj100% (1)
- Smoking CessationDocument4 pagesSmoking CessationAimee GutierrezNo ratings yet
- Project Idea NotesDocument3 pagesProject Idea NotesZiauddin IslamNo ratings yet
- Alcoholism Is A Broad Term For Problems WithDocument2 pagesAlcoholism Is A Broad Term For Problems WithAishwarya Senthil RajanNo ratings yet
- You Can Quit Smoking: Consumer GuideDocument15 pagesYou Can Quit Smoking: Consumer GuideBrian HunzikerNo ratings yet
- Assessment 2 EssayDocument6 pagesAssessment 2 EssayMudassar Gul Bin AshrafNo ratings yet
- Health and Fitness-SmokingDocument17 pagesHealth and Fitness-SmokingJenny Kongyy100% (1)
- Abby Steiert - Paper 08 08Document3 pagesAbby Steiert - Paper 08 08api-537004115No ratings yet
- Draft Tobacco Regulations For DaltonDocument18 pagesDraft Tobacco Regulations For DaltoniBerkshires.comNo ratings yet
- Tobacco Cessation Treatment PlanDocument7 pagesTobacco Cessation Treatment PlanyellowishmustardNo ratings yet
- Term Paper in English IV - BDocument18 pagesTerm Paper in English IV - BJai-JaiAdalidNo ratings yet
- 2016 SGR Full Report Non-508 PDFDocument298 pages2016 SGR Full Report Non-508 PDFkamalkumar15No ratings yet
- Full ReportDocument1,081 pagesFull ReportgmcatsupNo ratings yet
- Ecigarete Use Among Youth and Young AdultsDocument298 pagesEcigarete Use Among Youth and Young AdultsAsd EfgNo ratings yet
- HelpingsmokersquitDocument23 pagesHelpingsmokersquitapi-295416335No ratings yet
- Strategies and Design of Hypnosis Intervention ForDocument26 pagesStrategies and Design of Hypnosis Intervention ForClaudia AranedaNo ratings yet
- FC ProjectDocument6 pagesFC ProjectSufiyan Rangoonwala50% (2)
- Research Paper Smoking AddictionDocument4 pagesResearch Paper Smoking Addictionp1zajywigyd2100% (1)
- Smoking JournalDocument3 pagesSmoking Journaldamcon7No ratings yet
- Write A Thesis Statement Alcohol AbuseDocument8 pagesWrite A Thesis Statement Alcohol Abusejessicaspellfayetteville100% (2)
- 10 Drug and Alcohol Policies That Will Save LivesDocument4 pages10 Drug and Alcohol Policies That Will Save Livesmitmanta5433No ratings yet
- Step 3 - Drug AddictionDocument7 pagesStep 3 - Drug AddictionYagami ShmuelNo ratings yet
- Alcohol Abuse and AlcoholismDocument3 pagesAlcohol Abuse and Alcoholism890225No ratings yet
- Prevention of Substance AbuseDocument18 pagesPrevention of Substance AbuseAyur TadimallaNo ratings yet
- RRL LatestDocument21 pagesRRL LatestDino DizonNo ratings yet
- Reference Summary: X-Plain Smoking - Your ChoiceDocument4 pagesReference Summary: X-Plain Smoking - Your ChoiceNLNo ratings yet
- Plan of Care-Ashley BuccioDocument6 pagesPlan of Care-Ashley Buccioapi-597936486No ratings yet
- Factors Correlated With Smoking Cessation Success in Older Adults: A Retrospective Cohort Study in TaiwanDocument9 pagesFactors Correlated With Smoking Cessation Success in Older Adults: A Retrospective Cohort Study in TaiwanKhaziatun NurNo ratings yet
- Asac Action: Area Substance Abuse Council Board of DirectorsDocument4 pagesAsac Action: Area Substance Abuse Council Board of DirectorsUnited Way of East Central IowaNo ratings yet
- Sma08 4126Document40 pagesSma08 4126bjoaisdjofiwjeoijfiwNo ratings yet
- Benefits of Quitting Marijuana and A Timeline of Effects 2Document1 pageBenefits of Quitting Marijuana and A Timeline of Effects 2J PEYNo ratings yet
- Pittsfield Tobacco RegulationsDocument17 pagesPittsfield Tobacco RegulationsiBerkshires.comNo ratings yet
- Cigarette Smoking Interventions Among Diverse Populations: One of The Greatest Public Health Success Stories of The PastDocument8 pagesCigarette Smoking Interventions Among Diverse Populations: One of The Greatest Public Health Success Stories of The PastJeanet PrisiliaNo ratings yet
- A Mental Disorder or Mental Illness Is A Psychological Pattern or AnomalyDocument6 pagesA Mental Disorder or Mental Illness Is A Psychological Pattern or Anomalynavishana MalikNo ratings yet
- Cigarettes and Other Tobacco Products: How Does Tobacco Affect The Brain?Document6 pagesCigarettes and Other Tobacco Products: How Does Tobacco Affect The Brain?Monica MenaNo ratings yet
- Fseprd 531949Document2 pagesFseprd 531949Tee R TaylorNo ratings yet
- CrickettPartsList PDFDocument1 pageCrickettPartsList PDFTee R TaylorNo ratings yet
- 47 Ways To Hide Your GunsDocument21 pages47 Ways To Hide Your GunsRichard Andrianjaka LuckyNo ratings yet
- Masonery DM166Document10 pagesMasonery DM166freedom_lover_kNo ratings yet
- 2nd Devons Smle RifleDocument3 pages2nd Devons Smle RifleTee R TaylorNo ratings yet
- Odyssey 325 ST Davit Lifting ChocksDocument2 pagesOdyssey 325 ST Davit Lifting ChocksTee R TaylorNo ratings yet
- 3 Ways To Fight Fraud Ebook 083116Document9 pages3 Ways To Fight Fraud Ebook 083116Tee R TaylorNo ratings yet
- Chromatic Sans ManualDocument24 pagesChromatic Sans ManualTee R TaylorNo ratings yet
- APG3004D ManualDocument13 pagesAPG3004D ManualTee R TaylorNo ratings yet
- Fiji CommerceDocument38 pagesFiji CommerceTee R TaylorNo ratings yet
- Colorado LandsDocument60 pagesColorado LandsTee R TaylorNo ratings yet
- Colorado LandsDocument60 pagesColorado LandsTee R TaylorNo ratings yet
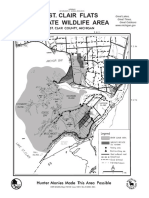
- ST Clair Flats SWA MapDocument2 pagesST Clair Flats SWA MapTee R TaylorNo ratings yet
- Fiji CommerceDocument38 pagesFiji CommerceTee R TaylorNo ratings yet
- Mississippi National ForestDocument31 pagesMississippi National ForestTee R TaylorNo ratings yet
- Colorado LandsDocument60 pagesColorado LandsTee R TaylorNo ratings yet
- Fiji CommerceDocument38 pagesFiji CommerceTee R TaylorNo ratings yet
- Fiji CommerceDocument38 pagesFiji CommerceTee R TaylorNo ratings yet
- 1105 IllusionsDocument6 pages1105 IllusionsHernando RiojaNo ratings yet
- Letters of ComplaintDocument3 pagesLetters of ComplaintMercedes Jimenez RomanNo ratings yet
- Data Sheet Physics 1 Module 10BDocument2 pagesData Sheet Physics 1 Module 10BBryanHarold BrooNo ratings yet
- Tips On Being A Successful StudentDocument2 pagesTips On Being A Successful Studentshimbir100% (3)
- Food Corporation of India Zonal Office (N) A-2A, 2B, SECTOR-24, NOIDADocument34 pagesFood Corporation of India Zonal Office (N) A-2A, 2B, SECTOR-24, NOIDAEpaper awaazNo ratings yet
- Physiotherapy For ChildrenDocument2 pagesPhysiotherapy For ChildrenCatalina LucaNo ratings yet
- Integrating Intuition and Analysis Edward Deming Once SaidDocument2 pagesIntegrating Intuition and Analysis Edward Deming Once SaidRimsha Noor ChaudaryNo ratings yet
- Parathyroid Agents PDFDocument32 pagesParathyroid Agents PDFRhodee Kristine DoñaNo ratings yet
- Thermal ComfortDocument6 pagesThermal ComfortHoucem Eddine MechriNo ratings yet
- Comparative Analysis of Levis Wrangler & LeeDocument10 pagesComparative Analysis of Levis Wrangler & LeeNeelakshi srivastavaNo ratings yet
- Security and Azure SQL Database White PaperDocument15 pagesSecurity and Azure SQL Database White PaperSteve SmithNo ratings yet
- Program PlanningDocument24 pagesProgram Planningkylexian1No ratings yet
- SSP ReviwerDocument40 pagesSSP ReviwerRick MabutiNo ratings yet
- Modern State and Contemporaray Global GovernanceDocument34 pagesModern State and Contemporaray Global GovernancePhoebe BuffayNo ratings yet
- Spoken KashmiriDocument120 pagesSpoken KashmiriGourav AroraNo ratings yet
- Simple Past Story 1Document7 pagesSimple Past Story 1Ummi Umarah50% (2)
- A Re Ection On The Dominant Learning Theories: Behaviourism, Cognitivism and ConstructivismDocument13 pagesA Re Ection On The Dominant Learning Theories: Behaviourism, Cognitivism and Constructivismchill protocolNo ratings yet
- K Unit 1 SeptemberDocument2 pagesK Unit 1 Septemberapi-169447826No ratings yet
- Icmap Newsletter June 2017Document7 pagesIcmap Newsletter June 2017GoopNo ratings yet
- Caucasus University Caucasus Doctoral School SyllabusDocument8 pagesCaucasus University Caucasus Doctoral School SyllabusSimonNo ratings yet
- ENVSOCTY 1HA3 - Lecture 01 - Introduction & Course Overview - Skeletal NotesDocument28 pagesENVSOCTY 1HA3 - Lecture 01 - Introduction & Course Overview - Skeletal NotesluxsunNo ratings yet
- Amy Kelaidis Resume Indigeous Education 2015 FinalDocument3 pagesAmy Kelaidis Resume Indigeous Education 2015 Finalapi-292414807No ratings yet