You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Psychometric Success Abstract ReasoningDocument73 pagesPsychometric Success Abstract ReasoningLea Foy-os Capili100% (12)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
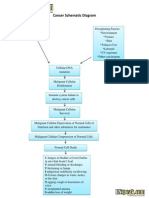
- Cancer Schematic DiagramDocument1 pageCancer Schematic DiagramCyrus De Asis100% (4)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- MS 2 - NCP Deep Vein ThrombosisDocument4 pagesMS 2 - NCP Deep Vein ThrombosisDominique Excelsis J. Degamo67% (3)
- IMPAC Tool for Making Pregnancy SaferDocument16 pagesIMPAC Tool for Making Pregnancy SaferLea Foy-os CapiliNo ratings yet
- Dengue Prevention CampaignDocument24 pagesDengue Prevention CampaignMuhammad Umer Abdullah100% (1)
- Community Evaluation Exam 2022Document11 pagesCommunity Evaluation Exam 2022Ryan-Jay Abolencia100% (1)
- Faktor-Faktor Yang Mempengaruhi Tuberculosis Multidrug Resistance (TB MDR)Document9 pagesFaktor-Faktor Yang Mempengaruhi Tuberculosis Multidrug Resistance (TB MDR)Dian RohmayantiNo ratings yet
- Getting inspired about oxygen delivery devicesDocument4 pagesGetting inspired about oxygen delivery devicesTubagus HidayatullahNo ratings yet
- Interpret ABGs with this 38-characterDocument1 pageInterpret ABGs with this 38-characterLea Foy-os Capili100% (1)
- Battle Against LeukemiaDocument30 pagesBattle Against LeukemiaLea Foy-os CapiliNo ratings yet
- The Hail, Holy Queen:: Additional PrayersDocument5 pagesThe Hail, Holy Queen:: Additional PrayersLea Foy-os CapiliNo ratings yet
- HAAD RequirementsDocument2 pagesHAAD RequirementsLea Foy-os Capili75% (4)
- TB MGTDocument3 pagesTB MGTLea Foy-os CapiliNo ratings yet
- Holy Rosary PDFDocument1 pageHoly Rosary PDFleslie_francisco_1No ratings yet
- Arrival and Taking The Exam at The Test CentreDocument2 pagesArrival and Taking The Exam at The Test CentreLea Foy-os CapiliNo ratings yet
- Sa Jan12 CbeDocument4 pagesSa Jan12 CbemzahidbNo ratings yet
- HAAD RequirementsDocument2 pagesHAAD RequirementsLea Foy-os Capili75% (4)
- Policy For Issuing Temporary Permits For Registered NursesDocument2 pagesPolicy For Issuing Temporary Permits For Registered NursesLea Foy-os CapiliNo ratings yet
- General Study TipsDocument4 pagesGeneral Study TipsLea Foy-os CapiliNo ratings yet
- MS Notes 1Document8 pagesMS Notes 1Lea Foy-os CapiliNo ratings yet
- Children Language DevtDocument4 pagesChildren Language DevtLea Foy-os CapiliNo ratings yet
- 1 s2.0 S0165032715001184 MainDocument6 pages1 s2.0 S0165032715001184 MainWirawan AdikusumaNo ratings yet
- Importance of Physical Activity and Preventing Communicable DiseasesDocument2 pagesImportance of Physical Activity and Preventing Communicable DiseasesMelrose LopezNo ratings yet
- CDC 118387 DS1Document132 pagesCDC 118387 DS1Sina AyodejiNo ratings yet
- Louisiana Couple Sues Pelahatchie Water Park After Daughter Allegedly Contracts E. ColiDocument9 pagesLouisiana Couple Sues Pelahatchie Water Park After Daughter Allegedly Contracts E. ColiWLBT NewsNo ratings yet
- COMMUNITY HEALTH ProjectDocument5 pagesCOMMUNITY HEALTH ProjectRana AlaseeriNo ratings yet
- Vaccines Reading ComprehensionDocument2 pagesVaccines Reading ComprehensionYolanda RamonNo ratings yet
- Letter To Parents From Southside ISDDocument2 pagesLetter To Parents From Southside ISDCody KingNo ratings yet
- Register Kunjungan Pasien BPJSDocument7 pagesRegister Kunjungan Pasien BPJSLuLu Ika RizkikaNo ratings yet
- Questions and Answers: MumpsDocument4 pagesQuestions and Answers: MumpsHannahNo ratings yet
- Epidemiology of ObesityDocument32 pagesEpidemiology of ObesityamsabavanNo ratings yet
- Block K Distribution by MMCDocument6 pagesBlock K Distribution by MMCMuhammad FaizanNo ratings yet
- Mobile Phones and HealthDocument255 pagesMobile Phones and HealthID100% (1)
- Early Diagnosis of NeoplasisDocument25 pagesEarly Diagnosis of NeoplasisDanielaNo ratings yet
- HIV/AIDS Document Explains Virus and DiseaseDocument38 pagesHIV/AIDS Document Explains Virus and DiseaseFarhan Herjanto100% (1)
- Jiang Et Al-2020-Journal of General Internal Medicine1Document6 pagesJiang Et Al-2020-Journal of General Internal Medicine1Farida MurtianiNo ratings yet
- 200-Article Text-1119-1-10-20200603Document6 pages200-Article Text-1119-1-10-20200603miaNo ratings yet
- Antibiotic Susceptibility Patterns of Methicillin Resistant Staphyl - PDF NIHDocument5 pagesAntibiotic Susceptibility Patterns of Methicillin Resistant Staphyl - PDF NIHzia ul RahmanNo ratings yet
- Live Experiences of OFW Seafarers Covid Survivors This PandemicDocument5 pagesLive Experiences of OFW Seafarers Covid Survivors This PandemicParong, AallyjahNo ratings yet
- Daftar PustakaDocument2 pagesDaftar PustakatiarNo ratings yet
- Sars-Cov-2 Variant of Concern Omicron: Update OnDocument24 pagesSars-Cov-2 Variant of Concern Omicron: Update OnDanna AflahNo ratings yet
- Pulse PressureDocument3 pagesPulse PressureYovie Anggara SaputraNo ratings yet
- Vaccination: DR Hodan Ahmed, MBBS, Mmed, Depr of Pediatrics, Amoud Medical School, AuDocument13 pagesVaccination: DR Hodan Ahmed, MBBS, Mmed, Depr of Pediatrics, Amoud Medical School, Auabdisalaan hassanNo ratings yet
- EpiDocument3 pagesEpiNiño PaoloNo ratings yet
- Jurnal Maternitas Ibu HamilDocument8 pagesJurnal Maternitas Ibu HamilriswandaNo ratings yet
- For COVID Patient This Acupressure Points May HelpsDocument51 pagesFor COVID Patient This Acupressure Points May HelpsNaidu Vegi100% (1)