You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- What Types of Benefits Does California Workers' Compensation Pay?Document5 pagesWhat Types of Benefits Does California Workers' Compensation Pay?Mona DeldarNo ratings yet
- PREFACE: " Chronic Fatigue Syndrome: A Guide To The Homeopathic Treatment of CFS/M.E."Document5 pagesPREFACE: " Chronic Fatigue Syndrome: A Guide To The Homeopathic Treatment of CFS/M.E."Diane SolomonNo ratings yet
- Pharmacy DC Pharmacy Laws and RegulationsDocument430 pagesPharmacy DC Pharmacy Laws and RegulationsTanganGondrongNo ratings yet
- Summary of Key Points from 2010 NHS White PaperDocument5 pagesSummary of Key Points from 2010 NHS White Paperdub2746No ratings yet
- Pharma Conpanies in Africa RegionDocument25 pagesPharma Conpanies in Africa RegionSiddhesh LawandeNo ratings yet
- Practicum ReportDocument33 pagesPracticum ReportPrivilege T Murambadoro100% (2)
- Application Post Basic BSC Nursing Gujarat AlpeshDocument4 pagesApplication Post Basic BSC Nursing Gujarat Alpeshacs888No ratings yet
- bsb301 New ProDocument7 pagesbsb301 New ProJasleen SohalNo ratings yet
- PHD Thesis by Publication - MD IRTEJA ISLAM - 0061107404 - 200521Document228 pagesPHD Thesis by Publication - MD IRTEJA ISLAM - 0061107404 - 200521Tanvir Ahmed NayeemNo ratings yet
- A Case Report: Hypersensitivity Reaction To DrugsDocument5 pagesA Case Report: Hypersensitivity Reaction To DrugsGNNo ratings yet
- Hubungan Response Time Perawat dan Keberhasilan Penanganan Pasien EmergencyDocument9 pagesHubungan Response Time Perawat dan Keberhasilan Penanganan Pasien Emergencysyaroh fatihatunnisaNo ratings yet
- NCCN Pain ManagementDocument14 pagesNCCN Pain ManagementcoooleNo ratings yet
- Ncm-106-Nursing-Process - Part3w1Document5 pagesNcm-106-Nursing-Process - Part3w1Marielle ChuaNo ratings yet
- PDFDocument70 pagesPDFPaul Benjomin AgregadoNo ratings yet
- Doctor-Patient Relationship - Cultural Aspects and Other Issues - Adel Adly RaghebDocument10 pagesDoctor-Patient Relationship - Cultural Aspects and Other Issues - Adel Adly RaghebAdel AdlyNo ratings yet
- Jenis Penelitian Dalam KebidananDocument95 pagesJenis Penelitian Dalam KebidananikaNo ratings yet
- IHI NSC Declaration To Advance Patient SafetyDocument12 pagesIHI NSC Declaration To Advance Patient SafetyAnonymous 4gmLmemTPNo ratings yet
- TR Implementation On The Support To DOHNCIPDILG JMC 2013 0103072022123435Document25 pagesTR Implementation On The Support To DOHNCIPDILG JMC 2013 0103072022123435azereth bartonNo ratings yet
- Criticalcare Positionpaper 060114Document25 pagesCriticalcare Positionpaper 060114BillaMozaNo ratings yet
- Diamond Select Ingenuity 128Document2 pagesDiamond Select Ingenuity 128Sepak OdokNo ratings yet
- Staffing: Roles & FunctionDocument12 pagesStaffing: Roles & FunctionfarizNo ratings yet
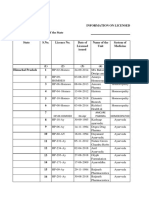
- Himachal Pradesh Aayush ListDocument9 pagesHimachal Pradesh Aayush ListplanetsandtarotNo ratings yet
- Exclusive Interview With Prof. V. K. CHAUHANDocument5 pagesExclusive Interview With Prof. V. K. CHAUHANHomoeopathic PulseNo ratings yet
- 11.initial Assesment & Stabilization of Poly Trauma PatientsDocument7 pages11.initial Assesment & Stabilization of Poly Trauma PatientsmyscribeNo ratings yet
- Health Quiz No. 2 TitleDocument2 pagesHealth Quiz No. 2 TitleLove LeiNo ratings yet
- Updated Resume DKDocument5 pagesUpdated Resume DKDK Aquino GomezNo ratings yet
- CHN CHP 8Document4 pagesCHN CHP 8Charmaine Rose Inandan Triviño75% (4)
- Osp Project Powerpoint Nurs 440Document20 pagesOsp Project Powerpoint Nurs 440api-101279115No ratings yet
- DLC BSH Public Report 3.13.2024Document87 pagesDLC BSH Public Report 3.13.2024Boston 25 DeskNo ratings yet
- Prevalence of Adentia in The Elderly and Development FactorsDocument4 pagesPrevalence of Adentia in The Elderly and Development FactorsCentral Asian StudiesNo ratings yet