You might also like
- Playwin Claim FormDocument3 pagesPlaywin Claim FormRajesh K SinghNo ratings yet
- Cancellation FormDocument2 pagesCancellation FormAkash TebaliyaNo ratings yet
- Axis Bank Personal Refund FormDocument1 pageAxis Bank Personal Refund FormSri Ram100% (1)
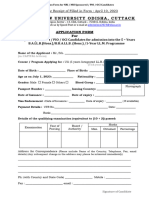
- Admission Form Nri Nris Pio Oci 2023Document3 pagesAdmission Form Nri Nris Pio Oci 2023zahirak345No ratings yet
- Supplementary FormDocument1 pageSupplementary Formdgauditsouth1632No ratings yet
- Application Form For World Passport, World Birth Card, World Birth Certificate, & World Identity CardDocument3 pagesApplication Form For World Passport, World Birth Card, World Birth Certificate, & World Identity CardLawrence Sweeting Jr.No ratings yet
- Application For Debit CardnewDocument2 pagesApplication For Debit CardnewSankalp KumarNo ratings yet
- Axis Forex New Refund FormDocument1 pageAxis Forex New Refund FormJaswanth ChandraNo ratings yet
- CS Form 100 - Revised 2015 - Final - Nov 6 2015Document2 pagesCS Form 100 - Revised 2015 - Final - Nov 6 2015Amur Jessica Bartolome FuentesNo ratings yet
- Form CPFMCDocument4 pagesForm CPFMCJeyavikinesh SelvakkuganNo ratings yet
- Birth FormDocument4 pagesBirth FormrahulNo ratings yet
- Application Form - InternationalDocument2 pagesApplication Form - InternationalMehak RaniNo ratings yet
- Vijana Baharia Loan Application Form FinalDocument9 pagesVijana Baharia Loan Application Form FinalkibeNo ratings yet
- Last First Middle InitialDocument3 pagesLast First Middle InitialAsjsjsjsNo ratings yet
- IdentityNotary FormDocument1 pageIdentityNotary Formkramergeorgec397No ratings yet
- Authorization To Use Credit CardDocument1 pageAuthorization To Use Credit CardAnna OgfNo ratings yet
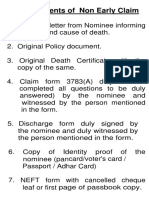
- Non Early Death Claim RequirementsDocument8 pagesNon Early Death Claim Requirementsrasiya49No ratings yet
- Application For Lottery Prize ClaimDocument3 pagesApplication For Lottery Prize ClaimAMit PrasadNo ratings yet
- Application AmexDocument8 pagesApplication AmexAkash HimuNo ratings yet
- ASET Recruit JOBS FormDocument4 pagesASET Recruit JOBS FormmuhammadimranavanNo ratings yet
- 2019 Chicago Marathon Waiver and Commitment Form - Guaranteed ExDocument3 pages2019 Chicago Marathon Waiver and Commitment Form - Guaranteed ExSeanSean ParkNo ratings yet
- Bharat Credit CardDocument2 pagesBharat Credit Cardrizanaqvi0% (1)
- MHF Loan FormDocument9 pagesMHF Loan Formshayaltanisha198No ratings yet
- Og KOE6 MuDocument2 pagesOg KOE6 Muderpina fluttrNo ratings yet
- Axis Travel Currency Card - Refund Form: Transaction DetailsDocument1 pageAxis Travel Currency Card - Refund Form: Transaction Detailsraj_bn4uNo ratings yet
- MBI Worldwide, 101 N. Park Ave., Suite 200, Herrin, IL 62948 Toll-Free 866-275-4624Document4 pagesMBI Worldwide, 101 N. Park Ave., Suite 200, Herrin, IL 62948 Toll-Free 866-275-4624KatieNo ratings yet
- b2c Authorization Form TemplateDocument2 pagesb2c Authorization Form TemplateshahinaNo ratings yet
- Auto-Offer PSBANKDocument3 pagesAuto-Offer PSBANKAnna KristinaNo ratings yet
- Required Documents Under Ehsas ScholarshipDocument8 pagesRequired Documents Under Ehsas ScholarshipMoazam KhanNo ratings yet
- 1Document1 page1ajkdnfkjdhkjsndNo ratings yet
- Credit Card Authorization FormDocument1 pageCredit Card Authorization FormCory PowerNo ratings yet
- USCredit ApplicationDocument5 pagesUSCredit ApplicationFSO COMPRESORESNo ratings yet
- Authorization Form For Third Party Inquiries CLG - Unsecured Collections - Credit CardsDocument1 pageAuthorization Form For Third Party Inquiries CLG - Unsecured Collections - Credit CardsLavinia BNo ratings yet
- AA Claim FormDocument5 pagesAA Claim FormpenchanskyNo ratings yet
- Refund FeeDocument2 pagesRefund Feefahmadk6No ratings yet
- Used Cars For Sale Offer FormDocument3 pagesUsed Cars For Sale Offer FormRaymond GabrielNo ratings yet
- Form CPFLMDocument4 pagesForm CPFLMKrishnan JayaramanNo ratings yet
- AMS Client Services Agreement VFDocument5 pagesAMS Client Services Agreement VFGary AndersonNo ratings yet
- Lass Ndividual Ubscriber Year Year: MTNL Rust INEDocument4 pagesLass Ndividual Ubscriber Year Year: MTNL Rust INEmkauraNo ratings yet
- PNB 1054 Housing LN NDocument11 pagesPNB 1054 Housing LN NSajal KulshresthaNo ratings yet
- Customer ApplicationDocument1 pageCustomer Applicationchill mainNo ratings yet
- Credit Card Payment Authorization Form: Company NameDocument2 pagesCredit Card Payment Authorization Form: Company NameAntwain UtleyNo ratings yet
- Notary Id Verification FormDocument1 pageNotary Id Verification FormSandra BenjaminNo ratings yet
- DOA Template LCDocument10 pagesDOA Template LCYash Mit100% (1)
- Atm Application FormDocument1 pageAtm Application FormBii LeonardNo ratings yet
- PRC ID Application FormDocument1 pagePRC ID Application FormCristof80% (5)
- Bank of Baroda: Application Form For HOME LOANDocument12 pagesBank of Baroda: Application Form For HOME LOANpravinartwinNo ratings yet
- Duplicate SSC APPFORM 2022Document2 pagesDuplicate SSC APPFORM 2022Firoz ShaikNo ratings yet
- Proforma of ApplicationDocument3 pagesProforma of ApplicationAditya KumarNo ratings yet
- Proforma of ApplicationDocument3 pagesProforma of ApplicationAditya KumarNo ratings yet
- Metro Insurance FormDocument2 pagesMetro Insurance FormMia Jackson100% (1)
- Affix Your Photo: Company ConfidentialDocument3 pagesAffix Your Photo: Company ConfidentialseventhhemanthNo ratings yet
- Deed of IndemnityDocument4 pagesDeed of IndemnityDhez ReyesNo ratings yet
- Registered Physician Assistant Form 3Document2 pagesRegistered Physician Assistant Form 3imperiouxxNo ratings yet
- How to Make Your Credit Card Rights Work for You: Save MoneyFrom EverandHow to Make Your Credit Card Rights Work for You: Save MoneyNo ratings yet
- Credit Report Secrets: How to Understand What Your Credit Report Says About You and What You Can Do About It!From EverandCredit Report Secrets: How to Understand What Your Credit Report Says About You and What You Can Do About It!Rating: 1 out of 5 stars1/5 (1)
- Farrell DobbsDocument15 pagesFarrell Dobbsjoallan123No ratings yet
- Pengetahuan UmumDocument681 pagesPengetahuan Umumsofta novaNo ratings yet
- Leadership Style of Raul RocoDocument25 pagesLeadership Style of Raul RocoRadee King CorpuzNo ratings yet
- Constitution Kelowna-Lake Country EDADocument12 pagesConstitution Kelowna-Lake Country EDAKelownaLiberalsNo ratings yet
- cs14 2013Document3 pagescs14 2013stephin k jNo ratings yet
- PEPSI Cola Vs TanauanDocument2 pagesPEPSI Cola Vs TanauanJimNo ratings yet
- Marine Advisors With The Vietnamese Provencial Reconnaissance Units 1966-1970Document85 pagesMarine Advisors With The Vietnamese Provencial Reconnaissance Units 1966-1970Bob Andrepont100% (4)
- Ulster County Industrial Development Agency - March 14, 2012 MinutesDocument8 pagesUlster County Industrial Development Agency - March 14, 2012 MinutesNewPaltzCurrentNo ratings yet
- EIT/LSIT Certification: Information and Application (Engineer-in-Training/Land Surveyor-in-Training)Document3 pagesEIT/LSIT Certification: Information and Application (Engineer-in-Training/Land Surveyor-in-Training)Ryan De Vera PagalNo ratings yet
- Digest Gonzales vs. Pennisi 614 SCRA 292 (2010) G.R. No. 169958Document4 pagesDigest Gonzales vs. Pennisi 614 SCRA 292 (2010) G.R. No. 169958KRDP ABCDNo ratings yet
- Tan Vs PerenaDocument2 pagesTan Vs PerenaPio Guieb AguilarNo ratings yet
- Depsrtment @lucatior: VacchatlonDocument3 pagesDepsrtment @lucatior: VacchatlonLeilani JuachonNo ratings yet
- Americké Voľby - PredikcieDocument1 pageAmerické Voľby - PredikciehnkyNo ratings yet
- Legal Research Writing Syllabus FinalDocument5 pagesLegal Research Writing Syllabus Finalremil badolesNo ratings yet
- 0241JICA (2006) Pakistan Transport Plan Study in The Islamic Republic of PakistanDocument330 pages0241JICA (2006) Pakistan Transport Plan Study in The Islamic Republic of Pakistankwazir70100% (1)
- United States Court of Appeals, Second Circuit.: No. 79. Docket 23183Document4 pagesUnited States Court of Appeals, Second Circuit.: No. 79. Docket 23183Scribd Government DocsNo ratings yet
- Moot Court Memorial On Behalf of RespondentsDocument19 pagesMoot Court Memorial On Behalf of RespondentsMAYUKH PARIALNo ratings yet
- Consti II Case ListDocument44 pagesConsti II Case ListGeron Gabriell SisonNo ratings yet
- Khyber Pakhtunkhwa Public Service CommissionDocument2 pagesKhyber Pakhtunkhwa Public Service CommissionazmatNo ratings yet
- Ras PDFDocument3 pagesRas PDFPadgro Consultants Pvt Ltd - EngineeringNo ratings yet
- Duncano Vs SandiganbayanDocument3 pagesDuncano Vs SandiganbayanGretch PanoNo ratings yet
- Global Royalties, Ltd. Et Al v. Xcentric Ventures, LLC Et Al - Document No. 23Document6 pagesGlobal Royalties, Ltd. Et Al v. Xcentric Ventures, LLC Et Al - Document No. 23Justia.comNo ratings yet
- Chapter Xiii: Department of Public Enterprises: 13.1.1 Irregular Payment To EmployeesDocument6 pagesChapter Xiii: Department of Public Enterprises: 13.1.1 Irregular Payment To EmployeesbawejaNo ratings yet
- Grade Sheet S: Final Examination, BBA ProgramDocument2 pagesGrade Sheet S: Final Examination, BBA ProgramRakib Hasan NirobNo ratings yet
- Distributive JusticeDocument8 pagesDistributive JusticethomasrblNo ratings yet
- 02 PSIR MAins 2019 Shubhra RanjanDocument9 pages02 PSIR MAins 2019 Shubhra Ranjanhard020% (1)
- Election Result Apsea 2022 23Document1 pageElection Result Apsea 2022 23sohaib sangiNo ratings yet
- Constitution of Pakistan: Relations Between Federation and ProvincesDocument11 pagesConstitution of Pakistan: Relations Between Federation and ProvincesSuhrab Khan JamaliNo ratings yet
- Legislative Department Case DigestDocument10 pagesLegislative Department Case DigestiyangtotNo ratings yet
- Statutes in EnglishDocument84 pagesStatutes in EnglishzulhakimNo ratings yet