You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Catheterization and EnemaDocument49 pagesCatheterization and EnemakhaimahalenylenNo ratings yet
- Intravenous Therapy Notes OnlineDocument5 pagesIntravenous Therapy Notes OnlineDexie James Ventenilla DizonNo ratings yet
- MasturbatrixDocument33 pagesMasturbatrixAndrée MajdNo ratings yet
- Final Questionnaires 123Document2 pagesFinal Questionnaires 123Kristel Jane QuitoNo ratings yet
- Fundam Nursing Skill Lab ManualDocument97 pagesFundam Nursing Skill Lab ManualBirhanu AyenewNo ratings yet
- Central Venous CatheterizationDocument34 pagesCentral Venous CatheterizationMujeeb NangrajNo ratings yet
- CBI Procedure Guide for NursesDocument9 pagesCBI Procedure Guide for NursesAlvin OccianoNo ratings yet
- Surgery Illustrated - Surgical Atlas: Mainz Pouch Continent Cutaneous DiversionDocument25 pagesSurgery Illustrated - Surgical Atlas: Mainz Pouch Continent Cutaneous DiversionAbdullah Bangwar100% (1)
- Urinary Catheterization Procedure ProtocolDocument10 pagesUrinary Catheterization Procedure Protocolmaha candraNo ratings yet
- Types of Catheters ExplainedDocument2 pagesTypes of Catheters ExplainedRocco WalksNo ratings yet
- CVC Partner 1Document40 pagesCVC Partner 1stefani83No ratings yet
- Centrel Venous CatheterizationDocument77 pagesCentrel Venous CatheterizationAli100% (1)
- Conversation ExerciseDocument4 pagesConversation ExerciseMbarr DiantoeNo ratings yet
- Precepted Clinical Skills Checklist Pre Experience (Medical/Surgical, ICU, ED, Telemetry Unit, or Psychiatry)Document9 pagesPrecepted Clinical Skills Checklist Pre Experience (Medical/Surgical, ICU, ED, Telemetry Unit, or Psychiatry)alyza lumpodNo ratings yet
- Department of Nursing: AssessmentDocument2 pagesDepartment of Nursing: Assessmentjoshua canjaNo ratings yet
- DextronixCatalog 0113bDocument15 pagesDextronixCatalog 0113bRóbert ŽuffaNo ratings yet
- Gap Analysis ISO 8836 2019Document27 pagesGap Analysis ISO 8836 2019suman100% (1)
- Nursing Students Practice Advanced SkillsDocument41 pagesNursing Students Practice Advanced SkillsMarcia AlmeidaNo ratings yet
- Central Line Associated Blood Stream Infection: Team 3: Cercado, Chiong, EsperidaDocument28 pagesCentral Line Associated Blood Stream Infection: Team 3: Cercado, Chiong, EsperidaJuniferNo ratings yet
- Lap Juli 2019Document144 pagesLap Juli 2019Asrina Ambo RakkaNo ratings yet
- Bladder IrrigationDocument9 pagesBladder IrrigationWelas_Riyanto_9968No ratings yet
- Fogarty Clot ManagementDocument3 pagesFogarty Clot Managementshreyas100% (1)
- Level III Performance Checklist: Preparing A Sterile Field: Using A Commercially Prepared Sterile Kit/Tray PurposeDocument40 pagesLevel III Performance Checklist: Preparing A Sterile Field: Using A Commercially Prepared Sterile Kit/Tray PurposeRichmon SantosNo ratings yet
- Peritoneal Dialysis Brochure US 401067001 A PDFDocument6 pagesPeritoneal Dialysis Brochure US 401067001 A PDFstaryk0% (1)
- Care and Management of Central Venous Catheters Policy - HH 1 .Ic.635.13Document52 pagesCare and Management of Central Venous Catheters Policy - HH 1 .Ic.635.13arisastraNo ratings yet
- Naso Oro SuctioningDocument4 pagesNaso Oro SuctioningandreabreeNo ratings yet
- Pull Through PsarpDocument3 pagesPull Through PsarphverdianNo ratings yet
- Certificate of Analysis: Suzhou Yaxin Medical Products Co., LTDDocument2 pagesCertificate of Analysis: Suzhou Yaxin Medical Products Co., LTDVictor AlarcónNo ratings yet
- Vascular Snare Family Brochure W. MicroDocument4 pagesVascular Snare Family Brochure W. MicroRedhwan Abdullah qaid AlshubiNo ratings yet
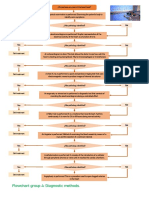
- Flowchart Group 4 Diagnostic Methods.Document1 pageFlowchart Group 4 Diagnostic Methods.Grupo 4 CardiologiaNo ratings yet