You might also like
- Physics For Entertainment Volume 1 (Yakov Perelman)Document211 pagesPhysics For Entertainment Volume 1 (Yakov Perelman)snath7800No ratings yet
- Reso Course PlannerDocument2 pagesReso Course PlannerSnehasishGhosh100% (1)
- MPLS QAsDocument6 pagesMPLS QAsLaxman Shrestha100% (1)
- Journal Pre-Proof: ExploreDocument43 pagesJournal Pre-Proof: ExploreLuís CorreiaNo ratings yet
- FirmcusbDocument123 pagesFirmcusbAndry1975No ratings yet
- UI5 TrainingDocument110 pagesUI5 TrainingShailesh KumarNo ratings yet
- First Summative Test in Math 5 (First Quarter)Document1 pageFirst Summative Test in Math 5 (First Quarter)Marlene Tagavilla-Felipe Diculen100% (1)
- Concrete Compressive StrengthDocument4 pagesConcrete Compressive StrengthklynchelleNo ratings yet
- Efficacy of Retrowalking in Patients With Chronic Knee Osteoarthritis: A Single Group Experimental Pilot StudyDocument9 pagesEfficacy of Retrowalking in Patients With Chronic Knee Osteoarthritis: A Single Group Experimental Pilot StudyDr. Krishna N. SharmaNo ratings yet
- 21sankarlingam EtalDocument5 pages21sankarlingam EtaleditorijmrhsNo ratings yet
- Physiotherapy: P. Ratan Khuman Lourembam Surbala Priyanka Patel Dhara ChavdaDocument4 pagesPhysiotherapy: P. Ratan Khuman Lourembam Surbala Priyanka Patel Dhara ChavdaSahithya MNo ratings yet
- Post-Operative Clinical Outcomes in Patients With or Without The Use of Tourniquet in Total Knee Replacement SurgeryDocument3 pagesPost-Operative Clinical Outcomes in Patients With or Without The Use of Tourniquet in Total Knee Replacement SurgerymunazilatulchasanahNo ratings yet
- A Comparative Study Between Joint Mobilization and Conventional Physiotherapy in Knee OsteoarthritisDocument4 pagesA Comparative Study Between Joint Mobilization and Conventional Physiotherapy in Knee OsteoarthritisInternational Journal of PhysiotherapyNo ratings yet
- Effects of Kinesiotherapy, Ultrasound and Electrotherapy in Management of Bilateral Knee Osteoarthritis: Prospective Clinical TrialDocument10 pagesEffects of Kinesiotherapy, Ultrasound and Electrotherapy in Management of Bilateral Knee Osteoarthritis: Prospective Clinical TrialDavid Alejandro Cavieres AcuñaNo ratings yet
- 12 Hall 2Document7 pages12 Hall 2Luis MiguelNo ratings yet
- Arthroscopic Hip Surgery With A Microfracture Procedure of The Hip: Clinical Outcomes With Two-Year Follow-UpDocument10 pagesArthroscopic Hip Surgery With A Microfracture Procedure of The Hip: Clinical Outcomes With Two-Year Follow-Upmoonwalker2099No ratings yet
- Extracorporeal Shock Wave Therapy VersusDocument7 pagesExtracorporeal Shock Wave Therapy VersusGiannis SaramantosNo ratings yet
- Choi 2012Document7 pagesChoi 2012bbiibibibibibibibibiNo ratings yet
- Article The Biomechanical Behavior of Distal Foot JointsDocument12 pagesArticle The Biomechanical Behavior of Distal Foot JointsAlessandro MedinaNo ratings yet
- Schuh 2011Document8 pagesSchuh 2011Francisco Castillo VázquezNo ratings yet
- Tascioglu Et Al 2010 Short Term Effectiveness of Ultrasound Therapy in Knee OsteoarthritisDocument10 pagesTascioglu Et Al 2010 Short Term Effectiveness of Ultrasound Therapy in Knee Osteoarthritiskrishnamunirajulu1028No ratings yet
- Effect of Kinesio Taping On Knee Symptoms in Patients With HemophiliaDocument10 pagesEffect of Kinesio Taping On Knee Symptoms in Patients With HemophiliaFrankChenNo ratings yet
- Aaa - THAMARA - Comparing Hot Pack, Short-Wave Diathermy, Ultrasound, and Tens On Isokinetic Strength, Pain and Functional StatusDocument9 pagesAaa - THAMARA - Comparing Hot Pack, Short-Wave Diathermy, Ultrasound, and Tens On Isokinetic Strength, Pain and Functional StatusBruno FellipeNo ratings yet
- High Reproducibility of A Novel Fixed Anterior DraDocument11 pagesHigh Reproducibility of A Novel Fixed Anterior DraXavi MartinezNo ratings yet
- 8Document1 page8Daniel GuevaraNo ratings yet
- Effect of Chinese Massage Tui Na On Isokinetic MusDocument7 pagesEffect of Chinese Massage Tui Na On Isokinetic MusRiyas KhanNo ratings yet
- The Effects of Ultrasound Imaging Visual Feedback During Toe-Spread-Out Exercise in Subjects With Hallux ValgusDocument9 pagesThe Effects of Ultrasound Imaging Visual Feedback During Toe-Spread-Out Exercise in Subjects With Hallux ValguskeradNo ratings yet
- Short-Wave Diathermy in The Treatment of Knee OsteoarthritisDocument10 pagesShort-Wave Diathermy in The Treatment of Knee Osteoarthritisapi-462099014No ratings yet
- Tui Na Musculo IsocineticoDocument7 pagesTui Na Musculo IsocineticoCristian Dionisio Barros OsorioNo ratings yet
- Prospective, Controlled & Randomized Study: With & Without Epiduroscopy AssistanceDocument1 pageProspective, Controlled & Randomized Study: With & Without Epiduroscopy AssistanceProf. Dr. Ahmed El MollaNo ratings yet
- 1 UsDocument7 pages1 UsJenny VibsNo ratings yet
- Use of Transcutaneous Electrical Nerve Stimulation Device in Early Osteoarthritis of The KneeDocument7 pagesUse of Transcutaneous Electrical Nerve Stimulation Device in Early Osteoarthritis of The KneeAlifah Nisrina Rihadatul AisyNo ratings yet
- 10 Jpts 27 1455Document3 pages10 Jpts 27 1455mustafasacarNo ratings yet
- Nice 1stDocument6 pagesNice 1staldiNo ratings yet
- F0602044753 PDFDocument7 pagesF0602044753 PDFArif Adi FatuhrokhmanNo ratings yet
- Outcome Assesment of Proximal Fibular Osteotomy in Medial Compartment Knee OsteoarthritisDocument3 pagesOutcome Assesment of Proximal Fibular Osteotomy in Medial Compartment Knee OsteoarthritisPrashant GuptaNo ratings yet
- Acupuntura para La RodillaDocument9 pagesAcupuntura para La Rodillaoscarin123456789No ratings yet
- Rehab ManualDocument11 pagesRehab ManualManoj KumarNo ratings yet
- Assessment of The Anterior Talofibular Ligament Thickness 2017 Journal of MeDocument5 pagesAssessment of The Anterior Talofibular Ligament Thickness 2017 Journal of MeRyana Fitriana IINo ratings yet
- The Effect of Mechanical Massage On Early Outcome After Total Knee ArthroplastyDocument4 pagesThe Effect of Mechanical Massage On Early Outcome After Total Knee Arthroplasty이용기No ratings yet
- 1 s2.0 S1607551X09703614 MainDocument8 pages1 s2.0 S1607551X09703614 MainAchenk BarcelonistaNo ratings yet
- Combined exercises more effective for osteoarthritis knee painDocument7 pagesCombined exercises more effective for osteoarthritis knee painirmarizkyyNo ratings yet
- Park 2014Document7 pagesPark 2014Nurfitrianti ArfahNo ratings yet
- Immediate Effects of 2 Types of Braces On Pain and Grip Strength in People With Lateral Epicondylalgia: A Randomized Controlled TrialDocument9 pagesImmediate Effects of 2 Types of Braces On Pain and Grip Strength in People With Lateral Epicondylalgia: A Randomized Controlled TrialRodrigo HamadaNo ratings yet
- Tendon 2Document10 pagesTendon 2Verónica Téllez ArriagaNo ratings yet
- International Journal of Health Sciences and ResearchDocument7 pagesInternational Journal of Health Sciences and ResearchMuhamad BenyaminNo ratings yet
- Pichon Naz 2016Document29 pagesPichon Naz 2016Williams Ariel Chandia PérezNo ratings yet
- Effects of Kinesiology Taping On Repositioning Error of The Knee Joint After Quadriceps Muscle FatigueDocument3 pagesEffects of Kinesiology Taping On Repositioning Error of The Knee Joint After Quadriceps Muscle FatigueYoga MatiinuNo ratings yet
- Arthroscopic Treatment of Acute Septic Arthritis After Meniscal Allograft TransplantationDocument4 pagesArthroscopic Treatment of Acute Septic Arthritis After Meniscal Allograft TransplantationserubimNo ratings yet
- Ultrasonographic Evaluation of Plantar Fasciitis After Low-Level Laser Therapy: Results of A Double-Blind, Randomized, Placebo-Controlled TrialDocument7 pagesUltrasonographic Evaluation of Plantar Fasciitis After Low-Level Laser Therapy: Results of A Double-Blind, Randomized, Placebo-Controlled TrialSri HariNo ratings yet
- 1 s2.0 S0003999319303892 MainDocument8 pages1 s2.0 S0003999319303892 MainRizkyrafiqoh afdinNo ratings yet
- tmp7403 TMPDocument2 pagestmp7403 TMPFrontiersNo ratings yet
- IJRR0029Document4 pagesIJRR0029Alice AmaratyaNo ratings yet
- Title:: Proforma For The Thesis of Master of SurgeryDocument17 pagesTitle:: Proforma For The Thesis of Master of SurgerySumit Kumar GuptaNo ratings yet
- Jpts 27 3355Document3 pagesJpts 27 3355Gabriel GonzalezNo ratings yet
- Clinical Study: Autologous Blood Injection and Wrist Immobilisation For Chronic Lateral EpicondylitisDocument6 pagesClinical Study: Autologous Blood Injection and Wrist Immobilisation For Chronic Lateral EpicondylitistriptykhannaNo ratings yet
- Laprade 2012Document11 pagesLaprade 2012Aaron BNo ratings yet
- Efek Pemberian Dynamic Splint Pada OA GenuDocument1 pageEfek Pemberian Dynamic Splint Pada OA GenuLisa NurhasanahNo ratings yet
- C Rioter ApyDocument6 pagesC Rioter ApyDanNy ClaudiuNo ratings yet
- The Study To Assess The Effect of Prehabilitation On Postoperative Outcome of The Patients On Total Knee Arthroplasty at Selected HospitalDocument4 pagesThe Study To Assess The Effect of Prehabilitation On Postoperative Outcome of The Patients On Total Knee Arthroplasty at Selected HospitalEditor IJTSRDNo ratings yet
- The efficacy of post‑operative devices following knee arthroscopic surgery a systematic reviewDocument16 pagesThe efficacy of post‑operative devices following knee arthroscopic surgery a systematic reviewfilipecorsairNo ratings yet
- Comparison Between Outcomes of Dry Needling With Conventional Protocol and Rood's Approach With Conventional Protocol On Pain, Strength and Balance in Knee OsteoarthritisDocument29 pagesComparison Between Outcomes of Dry Needling With Conventional Protocol and Rood's Approach With Conventional Protocol On Pain, Strength and Balance in Knee OsteoarthritisDrPratibha SinghNo ratings yet
- Effects of Walking With Blood Ow Restriction On Limb Venous Compliance in Elderly SubjectsDocument5 pagesEffects of Walking With Blood Ow Restriction On Limb Venous Compliance in Elderly SubjectsJonathan Alexis Salinas UlloaNo ratings yet
- International Journal of Osteopathic Medicine Volume 11 Issue 4 2008Document1 pageInternational Journal of Osteopathic Medicine Volume 11 Issue 4 2008Nuno CavaleiroNo ratings yet
- Original Article: Effects of Exercise Therapy For Knee OsteoarthritisDocument6 pagesOriginal Article: Effects of Exercise Therapy For Knee OsteoarthritisChristian NievesNo ratings yet
- Conservative Treatment of Thumb Base Osteoarthritis A Systematic Review 2015 The Journal of Hand SurgeryDocument12 pagesConservative Treatment of Thumb Base Osteoarthritis A Systematic Review 2015 The Journal of Hand SurgeryProfesseur Christian DumontierNo ratings yet
- Scientific Research Journal of India ScReJI Volume 7 Issue 2 Year 2023Document53 pagesScientific Research Journal of India ScReJI Volume 7 Issue 2 Year 2023Dr. Krishna N. SharmaNo ratings yet
- Scientific Research Journal of India SRJI Complete Vol-1 2012 All IssuesDocument233 pagesScientific Research Journal of India SRJI Complete Vol-1 2012 All IssuesDr. Krishna N. SharmaNo ratings yet
- Scientific Research Journal of India SRJI Complete Vol-5 2016-2021 All IssuesDocument30 pagesScientific Research Journal of India SRJI Complete Vol-5 2016-2021 All IssuesDr. Krishna N. SharmaNo ratings yet
- Physiotherapy Intervention in Management of Dizziness: Shahanawaz SDDocument11 pagesPhysiotherapy Intervention in Management of Dizziness: Shahanawaz SDDr. Krishna N. SharmaNo ratings yet
- Respiratory Physiotherapy in Triple Vessel Disease With Post Coronary Artery Bypass Grafting Surgery (CABG) SRJI Vol 2 Issue 3 Year 2013Document4 pagesRespiratory Physiotherapy in Triple Vessel Disease With Post Coronary Artery Bypass Grafting Surgery (CABG) SRJI Vol 2 Issue 3 Year 2013Dr. Krishna N. SharmaNo ratings yet
- Scientific Research Journal of India SRJI Complete Vol-4 2015 All IssuesDocument53 pagesScientific Research Journal of India SRJI Complete Vol-4 2015 All IssuesDr. Krishna N. SharmaNo ratings yet
- Evidence of Barriers To Evidence-Based Physiotherapy Practice in Northern AfricaDocument5 pagesEvidence of Barriers To Evidence-Based Physiotherapy Practice in Northern AfricaDr. Krishna N. SharmaNo ratings yet
- Mayank Pushkar. Congenital Talipes Equinovarus (CTEV) SRJI Vol - 2, Issue - 1, Year - 2013Document7 pagesMayank Pushkar. Congenital Talipes Equinovarus (CTEV) SRJI Vol - 2, Issue - 1, Year - 2013Dr. Krishna N. SharmaNo ratings yet
- Full Journal SRJI Volume-1 Issue-3 Year-2012 Scientific Research Journal of IndiaDocument81 pagesFull Journal SRJI Volume-1 Issue-3 Year-2012 Scientific Research Journal of IndiaDr. Krishna N. SharmaNo ratings yet
- Pranjal Parmar. Comparison of The Effect of Isometric Exercise of Upper Limb On Vitals Between Young Males and FemalesDocument13 pagesPranjal Parmar. Comparison of The Effect of Isometric Exercise of Upper Limb On Vitals Between Young Males and FemalesDr. Krishna N. SharmaNo ratings yet
- Parmar Sanjay T., Nayana A. Khobre. Growth in Cerebral Palsy Children Between 3-13 Years in Urban Dharwad, IndiaDocument7 pagesParmar Sanjay T., Nayana A. Khobre. Growth in Cerebral Palsy Children Between 3-13 Years in Urban Dharwad, IndiaDr. Krishna N. SharmaNo ratings yet
- Exploring The Roots of ElectrotherapyDocument4 pagesExploring The Roots of ElectrotherapyDr. Krishna N. SharmaNo ratings yet
- Impact of Ageing On Depression and Activities of Daily Livings in Normal Elderly Subjects Living in Old Age Homes and Communities of Kanpur, U.PDocument8 pagesImpact of Ageing On Depression and Activities of Daily Livings in Normal Elderly Subjects Living in Old Age Homes and Communities of Kanpur, U.PDr. Krishna N. SharmaNo ratings yet
- Occupational Therapy Marketing Indian Prospective SRJI Vol 2 Issue 3 Year 2013Document8 pagesOccupational Therapy Marketing Indian Prospective SRJI Vol 2 Issue 3 Year 2013Dr. Krishna N. SharmaNo ratings yet
- Ito Test: Does Height of The Pad Affect Back Muscle Endurance?Document7 pagesIto Test: Does Height of The Pad Affect Back Muscle Endurance?Dr. Krishna N. SharmaNo ratings yet
- Effects of Task Related Sitting Training On Balance in Hemiplegic Patients. Dr. Vivek H. Ramanandi Srji Vol 1 Issue 4 Year 2013Document9 pagesEffects of Task Related Sitting Training On Balance in Hemiplegic Patients. Dr. Vivek H. Ramanandi Srji Vol 1 Issue 4 Year 2013Dr. Krishna N. SharmaNo ratings yet
- Network Border Patrol Eradicates The Over Loading of Data Packets and Prevents Congestion Collapse Thereby Promoting Fairness Over TCP Protocol in LAN WAN SRJI Vol-1 Issue-1 Year-2013Document10 pagesNetwork Border Patrol Eradicates The Over Loading of Data Packets and Prevents Congestion Collapse Thereby Promoting Fairness Over TCP Protocol in LAN WAN SRJI Vol-1 Issue-1 Year-2013Dr. Krishna N. SharmaNo ratings yet
- Efficacy of Retrowalking in Patients With Chronic Knee Osteoarthritis: A Single Group Experimental Pilot StudyDocument9 pagesEfficacy of Retrowalking in Patients With Chronic Knee Osteoarthritis: A Single Group Experimental Pilot StudyDr. Krishna N. SharmaNo ratings yet
- Effectiveness of Conventional Physical Therapy & C.P.M Unit For Functional Rehabilitation After Total Knee ArthroplastyDocument21 pagesEffectiveness of Conventional Physical Therapy & C.P.M Unit For Functional Rehabilitation After Total Knee ArthroplastyDr. Krishna N. SharmaNo ratings yet
- Evidence of Barriers To Evidence-Based Physiotherapy Practice in Nothern AfricaDocument7 pagesEvidence of Barriers To Evidence-Based Physiotherapy Practice in Nothern AfricaDr. Krishna N. SharmaNo ratings yet
- Efficacy of 3D Gliding On Pain in Patients With Knee Osteoarthritis A Randomized Controlled Pilot StudyDocument5 pagesEfficacy of 3D Gliding On Pain in Patients With Knee Osteoarthritis A Randomized Controlled Pilot StudyDr. Krishna N. SharmaNo ratings yet
- Effect of Core Stabilization Training On Endurance of Trunk Extensor and Functional Capacity in Subjects With Mechanical Low Back PainDocument8 pagesEffect of Core Stabilization Training On Endurance of Trunk Extensor and Functional Capacity in Subjects With Mechanical Low Back PainDr. Krishna N. SharmaNo ratings yet
- Effectiveness of Supervised Graded Repetitive Arm Supplementary Program On Arm Function in Subjects With StrokeDocument10 pagesEffectiveness of Supervised Graded Repetitive Arm Supplementary Program On Arm Function in Subjects With StrokeDr. Krishna N. SharmaNo ratings yet
- Ethical Challenges For Occupational Therapist in India To Use Social MediaDocument6 pagesEthical Challenges For Occupational Therapist in India To Use Social MediaDr. Krishna N. SharmaNo ratings yet
- Effects of Bimanual Functional Practice Training On Functional Performance of Upper Extremity in Chronic Stroke SRJI Vol 2 Issue 3 Year 2013Document10 pagesEffects of Bimanual Functional Practice Training On Functional Performance of Upper Extremity in Chronic Stroke SRJI Vol 2 Issue 3 Year 2013Dr. Krishna N. SharmaNo ratings yet
- Effectiveness of Neuromotor Task Training Combined With Kinaesthetic Training in Children With Developmental Co - Ordination Disorder - A Randomised Trial SRJI Vol-1 Issue-1 Year-2013Document15 pagesEffectiveness of Neuromotor Task Training Combined With Kinaesthetic Training in Children With Developmental Co - Ordination Disorder - A Randomised Trial SRJI Vol-1 Issue-1 Year-2013Dr. Krishna N. SharmaNo ratings yet
- Effectiveness of Core Strengthening Exercises To Reduce Incidence of Side Strain Injury in Medium Pace BowlersDocument12 pagesEffectiveness of Core Strengthening Exercises To Reduce Incidence of Side Strain Injury in Medium Pace BowlersDr. Krishna N. SharmaNo ratings yet
- Editorial Vol 1 Issue 2. (Scientific Research Journal of India)Document2 pagesEditorial Vol 1 Issue 2. (Scientific Research Journal of India)Dr. Krishna N. SharmaNo ratings yet
- Editorial Srji Vol 3 Issue 2 Year 2014Document1 pageEditorial Srji Vol 3 Issue 2 Year 2014Dr. Krishna N. SharmaNo ratings yet
- EditorialDocument1 pageEditorialDr. Krishna N. SharmaNo ratings yet
- Types of Nuclear Reactors GuideDocument19 pagesTypes of Nuclear Reactors GuideUgur GuvenNo ratings yet
- Faculty of Engineering and Computing Sciences: Annexure-IDocument2 pagesFaculty of Engineering and Computing Sciences: Annexure-IAkshay MehtaNo ratings yet
- Guide For Dynamic Report Generator - EndsfsdfsdfsdfsdfDocument15 pagesGuide For Dynamic Report Generator - Endsfsdfsdfsdfsdfmtech structuresNo ratings yet
- 93C66 Microwire EepromDocument13 pages93C66 Microwire EepromadrianramonNo ratings yet
- The Importance of Calculators in Math ClassDocument6 pagesThe Importance of Calculators in Math Classchloe shanice bordiosNo ratings yet
- Inverse Laplace Transformation Ex 11 2 Umer Asghar MethodDocument34 pagesInverse Laplace Transformation Ex 11 2 Umer Asghar MethodSikandar Khan100% (1)
- Heba Hathout - The Old Hats ProblemDocument11 pagesHeba Hathout - The Old Hats ProblemKluff5878No ratings yet
- Same Denominator or Numerator Worksheet 1Document2 pagesSame Denominator or Numerator Worksheet 1Jenny KimNo ratings yet
- SMD Meter User's ManualDocument2 pagesSMD Meter User's ManuallucianoNo ratings yet
- Experimental Noize Guitar Set 1 Effects PedalDocument2 pagesExperimental Noize Guitar Set 1 Effects PedalSingani Titicaca100% (1)
- DPWH Design Assessment ChecklistDocument18 pagesDPWH Design Assessment ChecklistGeovanni DumpasanNo ratings yet
- 20-SDMS-02 Overhead Line Accessories PDFDocument102 pages20-SDMS-02 Overhead Line Accessories PDFMehdi SalahNo ratings yet
- Problem Set Ee8205 PDFDocument4 pagesProblem Set Ee8205 PDFksajjNo ratings yet
- UDP Control and Monitoring With PIC Microcontroller - StudentCompanion PDFDocument14 pagesUDP Control and Monitoring With PIC Microcontroller - StudentCompanion PDFVport PortNo ratings yet
- XXXXX: Important Instructions To ExaminersDocument21 pagesXXXXX: Important Instructions To ExaminersYogesh DumaneNo ratings yet
- Delphi Temp SensorDocument2 pagesDelphi Temp SensorAlways Super Gaming vatsal GehlotNo ratings yet
- Materi Welding Defect IIDocument64 pagesMateri Welding Defect IIsmartz inspectionNo ratings yet
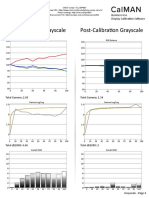
- TCL 55P607 CNET Review Calibration ResultsDocument3 pagesTCL 55P607 CNET Review Calibration ResultsDavid KatzmaierNo ratings yet
- MCQ Metrology (CCCM & CCCT) PDFDocument21 pagesMCQ Metrology (CCCM & CCCT) PDFSahil Gauhar67% (3)
- SUDOKU DocumentDocument37 pagesSUDOKU DocumentAmbika Sharma33% (3)
- The Pythagorean Spiral ProjectDocument2 pagesThe Pythagorean Spiral Projectapi-316478863No ratings yet
- ZF AVS Automatic Gearbox Manual PDFDocument67 pagesZF AVS Automatic Gearbox Manual PDFDardan HusiNo ratings yet