You might also like
- NHS Fife Assessment Chart For Wound ManagementDocument3 pagesNHS Fife Assessment Chart For Wound ManagementImran KhanNo ratings yet
- Wound Assessment ChartDocument4 pagesWound Assessment ChartSinichi Kudo100% (1)
- Wound Assessment ChartDocument2 pagesWound Assessment ChartAnonymous H3DpmCZX100% (6)
- Preventing Skin Damage and Pressure UlcersDocument29 pagesPreventing Skin Damage and Pressure UlcersJOSHUA DICHOSO100% (1)
- Pain Management in The Emergency: Dr. Prathiba Prasad Emergency Physician Masafi HospitalDocument50 pagesPain Management in The Emergency: Dr. Prathiba Prasad Emergency Physician Masafi HospitalPrathiba PrassaddNo ratings yet
- Pressure UlcerDocument35 pagesPressure Ulcerenam professor100% (1)
- Risk Assessment Chart - WaterlowDocument2 pagesRisk Assessment Chart - WaterlowRalucaNo ratings yet
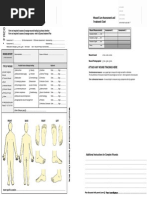
- Attach Any Wound Tracings Here Attach Any Wound Tracings HereDocument2 pagesAttach Any Wound Tracings Here Attach Any Wound Tracings Herewiwi handayani100% (1)
- ACLS Testing ChecklistDocument1 pageACLS Testing ChecklistmedcailinNo ratings yet
- Physical Assessment Lab Practice GuideDocument4 pagesPhysical Assessment Lab Practice GuideCatalina CortesNo ratings yet
- Lap Chole DictationDocument2 pagesLap Chole DictationAshish DongreNo ratings yet
- Peripheral IV Line ChecklistDocument3 pagesPeripheral IV Line Checklistaashika15100% (1)
- Recovery Room Transfer SheetDocument1 pageRecovery Room Transfer SheetDr. Sumit Kumbhar0% (1)
- Early Diagnosis & Prompt Treatment of Acute Abdominal PainDocument69 pagesEarly Diagnosis & Prompt Treatment of Acute Abdominal PainRani Silmi ZulafaNo ratings yet
- Role of Food and Its Medicinal ValueDocument9 pagesRole of Food and Its Medicinal Valueharshika tembhurneNo ratings yet
- Ot Instruments: Ms. Revathy. ADocument60 pagesOt Instruments: Ms. Revathy. AREVATHY.ANo ratings yet
- TriageDocument42 pagesTriageNic JiNo ratings yet
- Peripheral I.V. Line Checklist (Visual Infusion Phlebitis Score)Document1 pagePeripheral I.V. Line Checklist (Visual Infusion Phlebitis Score)aashika15100% (1)
- Mortuary admission formDocument1 pageMortuary admission formHrishikesh Kalgaonkar100% (1)
- Nursing ICUDocument2 pagesNursing ICUKomal Tomar50% (2)
- Pre Op ChecklistDocument1 pagePre Op ChecklistKoushik Reddy PodduturiNo ratings yet
- Case Sheet for Maternity ServicesDocument22 pagesCase Sheet for Maternity ServicesGulfeshan ArshiNo ratings yet
- Decubetic Ulcer (Bed Sores)Document22 pagesDecubetic Ulcer (Bed Sores)Jerry ZahidNo ratings yet
- Nursing care plan templateDocument1 pageNursing care plan templateRose Camille Delos Santos DatuinNo ratings yet
- Back CareDocument56 pagesBack CareSandeep Maan100% (2)
- Hospital Counseling FormDocument1 pageHospital Counseling FormBranding ShrimannHospitals100% (2)
- Types and Uses of Surgical NeedlesDocument12 pagesTypes and Uses of Surgical NeedlesAnuradha RoopchandNo ratings yet
- Federal Regulations of Pressure Sores (F314Document3 pagesFederal Regulations of Pressure Sores (F314Jing CruzNo ratings yet
- Blood Requisition FormDocument2 pagesBlood Requisition FormPrashant Kumar Singh100% (1)
- Preprocedure Check-In Sign-In Time-Out Sign-OutDocument2 pagesPreprocedure Check-In Sign-In Time-Out Sign-OutSyahri DzikriNo ratings yet
- Wong Baker's ScaleDocument3 pagesWong Baker's ScaleMalayNo ratings yet
- DVT Assessment FormDocument1 pageDVT Assessment FormLoy ZiNo ratings yet
- Vulnerable Patient Assessment CareDocument2 pagesVulnerable Patient Assessment CarePrabhat Kumar100% (1)
- 5 Labour Room Laqshya Assessment ToolkitDocument16 pages5 Labour Room Laqshya Assessment ToolkitAnjali Rahul Ajmeri50% (2)
- OSCE/OSPE EXAM GUIDEDocument51 pagesOSCE/OSPE EXAM GUIDELouise Tan100% (3)
- Strike Off Whichever Is Not ApplicableDocument1 pageStrike Off Whichever Is Not ApplicableSrisachidanand ShuklaNo ratings yet
- WOUND Assessment 1Document30 pagesWOUND Assessment 1Yunita BudiasmitasariNo ratings yet
- Transfer Hospital Choice FormDocument1 pageTransfer Hospital Choice FormAina Haravata100% (1)
- Cardiovascular System Assessment GuideDocument29 pagesCardiovascular System Assessment Guidesas100% (1)
- Self Declaration for Hospital EmpanelmentDocument12 pagesSelf Declaration for Hospital Empanelmentsrisaravanan100% (1)
- Operating Room Nurse Interview QuestionsDocument2 pagesOperating Room Nurse Interview Questionsali aliNo ratings yet
- Modified Glasgow Coma Scale For Infants and ChildrenDocument1 pageModified Glasgow Coma Scale For Infants and ChildrenYudha Perwira PutraNo ratings yet
- PATIENT PRE-OPERATIVE CHECKLISTDocument1 pagePATIENT PRE-OPERATIVE CHECKLISTАндрій ДанильцівNo ratings yet
- Diabetes Foot Examination FormDocument17 pagesDiabetes Foot Examination FormJANUAR RIZQINo ratings yet
- Pressure Ulcer Assessment Chart & Body MapDocument2 pagesPressure Ulcer Assessment Chart & Body MapWidfdsafdsaNo ratings yet
- Examination of Ulcer, Sinus & FistulaDocument8 pagesExamination of Ulcer, Sinus & FistulaManas RanjanNo ratings yet
- N.A.B.H. Parameter Sheet: Network Hospital Grading ProformaDocument7 pagesN.A.B.H. Parameter Sheet: Network Hospital Grading ProformaDhananjay SainiNo ratings yet
- Home Health Nursing AssessmentDocument2 pagesHome Health Nursing Assessmentjohn MNo ratings yet
- HKCAD Medical Report FormDocument4 pagesHKCAD Medical Report FormHelloWorldNo ratings yet
- Ssi Post Op FormDocument2 pagesSsi Post Op FormNewHopekilpauk HRNo ratings yet
- UHS Form No. 4 Health Examination Record - FORMDocument3 pagesUHS Form No. 4 Health Examination Record - FORMdNo ratings yet
- Wound Assessment: Pusat Perawatan Luka "Patria Care" Stikes Patria Husada BLITAR 2019Document54 pagesWound Assessment: Pusat Perawatan Luka "Patria Care" Stikes Patria Husada BLITAR 2019pristanti tantiNo ratings yet
- Wound CareDocument3 pagesWound CareAfenkNo ratings yet
- Clinical Assessment FormDocument17 pagesClinical Assessment FormBrittany Miley100% (1)
- Do Not Write Below This Line: Pamantasan NG Lungsod NG Maynila UHS Form No. 4Document3 pagesDo Not Write Below This Line: Pamantasan NG Lungsod NG Maynila UHS Form No. 4Harry AlegriaNo ratings yet
- Ortho EvaluationDocument82 pagesOrtho EvaluationMiti ThakkarNo ratings yet
- Chronic Leg Ulcers: Atef Abdel Hameed, MD Professor of Vascular Surgery Ain Shams UniversityDocument21 pagesChronic Leg Ulcers: Atef Abdel Hameed, MD Professor of Vascular Surgery Ain Shams UniversityAmr AbdelghaffarNo ratings yet
- Wound Assessment and DocumentationDocument7 pagesWound Assessment and DocumentationKana Ngai100% (2)
- Knee ArthrosDocument3 pagesKnee ArthrosBarney LivingstoneNo ratings yet
- Health Questionnaire - Occupational HealthDocument3 pagesHealth Questionnaire - Occupational HealthRJay JacabanNo ratings yet
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Colorado Revised Statutes (CRS 12 42.5) Title 12 Article 42.5 Professions and Occupations Pharmacists, Pharmacy Businesses, and PharmaceuticalsDocument48 pagesColorado Revised Statutes (CRS 12 42.5) Title 12 Article 42.5 Professions and Occupations Pharmacists, Pharmacy Businesses, and PharmaceuticalsBrian HarrisNo ratings yet
- Colorado Medical Use of Marijuana Department of Public Health and Environment Health and Environmental Information and Statistics Division 5 CCR 1006-2Document18 pagesColorado Medical Use of Marijuana Department of Public Health and Environment Health and Environmental Information and Statistics Division 5 CCR 1006-2Brian HarrisNo ratings yet
- Colorado Preferred Drug List (PDL) 2013Document25 pagesColorado Preferred Drug List (PDL) 2013Brian HarrisNo ratings yet
- Colorado CRS 18 18 - Uniform Controlled Substances Acto of 1992 Effective 7-1-2009Document69 pagesColorado CRS 18 18 - Uniform Controlled Substances Acto of 1992 Effective 7-1-2009Brian HarrisNo ratings yet
- Colorado CRS 18 18 - Uniform Controlled Substances Acto of 1992 Effective 7-1-2009Document69 pagesColorado CRS 18 18 - Uniform Controlled Substances Acto of 1992 Effective 7-1-2009Brian HarrisNo ratings yet
- Colorado Medical Use of Marijuana Revised Statutes 18-18-406.3Document2 pagesColorado Medical Use of Marijuana Revised Statutes 18-18-406.3Brian HarrisNo ratings yet
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Colorado Revised Statutes (CRS 12 36) Title 12 Article 36 and Article 36.5 Professions and Occupations, Medical Practice, Professional Review of Health Care ProvidersDocument57 pagesColorado Revised Statutes (CRS 12 36) Title 12 Article 36 and Article 36.5 Professions and Occupations, Medical Practice, Professional Review of Health Care ProvidersBrian HarrisNo ratings yet
- Colorado Peace Officer Manual 2013Document373 pagesColorado Peace Officer Manual 2013Brian Harris100% (1)
- Colorado Revised Statutes (CRS 12 12)Document65 pagesColorado Revised Statutes (CRS 12 12)Brian HarrisNo ratings yet
- Colorado Medical Board Policy Guidelines For The Use of Controlled Substances For The Treatment of Pain 12-36-117, C.R.S.Document5 pagesColorado Medical Board Policy Guidelines For The Use of Controlled Substances For The Treatment of Pain 12-36-117, C.R.S.Brian HarrisNo ratings yet
- Colorado Licensing of Controlled Substances Act 2013 Sunset ReviewDocument31 pagesColorado Licensing of Controlled Substances Act 2013 Sunset ReviewBrian HarrisNo ratings yet
- Colorado Drug Control UpdateDocument7 pagesColorado Drug Control UpdateBrian HarrisNo ratings yet
- Colorado Guidelines of Professional Practice For Controlled Substances AddendumDocument14 pagesColorado Guidelines of Professional Practice For Controlled Substances AddendumBrian HarrisNo ratings yet
- 42 CFR Part 8 Opioid Drugs in Maintenance and Detoxification Treatment of Opiate Addiction Final RuleDocument28 pages42 CFR Part 8 Opioid Drugs in Maintenance and Detoxification Treatment of Opiate Addiction Final RuleBrian HarrisNo ratings yet
- Colorado House Bill 11-1043 Concerning Medical Marijuana, and Making An Appropriation ThereforDocument24 pagesColorado House Bill 11-1043 Concerning Medical Marijuana, and Making An Appropriation ThereforBrian HarrisNo ratings yet
- Colorado Guidelines of Professional Practice For Controlled SubstancesDocument65 pagesColorado Guidelines of Professional Practice For Controlled SubstancesBrian HarrisNo ratings yet
- ASAM The Role of The Physician in "Medical" MarijuanaDocument60 pagesASAM The Role of The Physician in "Medical" MarijuanaBrian HarrisNo ratings yet
- Colorado Medical Board Policy Guidelines Pertaining To The Release and Retention of Medical Records Policy Number 40-07Document2 pagesColorado Medical Board Policy Guidelines Pertaining To The Release and Retention of Medical Records Policy Number 40-07Brian HarrisNo ratings yet
- Colorado Medical Marijuana Laws, Statutes, and CodesDocument60 pagesColorado Medical Marijuana Laws, Statutes, and CodesGreenpoint Insurance ColoradoNo ratings yet
- Colorado Guidelines of Professional Practice For Controlled Substances AddendumDocument14 pagesColorado Guidelines of Professional Practice For Controlled Substances AddendumBrian HarrisNo ratings yet
- Colorado Guidelines of Professional Practice For Controlled SubstancesDocument65 pagesColorado Guidelines of Professional Practice For Controlled SubstancesBrian HarrisNo ratings yet
- Colorado Revised Statutes (CRS 12 42.5) Title 12 Article 42.5 Professions and Occupations Pharmacists, Pharmacy Businesses, and PharmaceuticalsDocument48 pagesColorado Revised Statutes (CRS 12 42.5) Title 12 Article 42.5 Professions and Occupations Pharmacists, Pharmacy Businesses, and PharmaceuticalsBrian HarrisNo ratings yet
- Medical Injuries or Illnesses To Use Medical Marijuana in ColoradoDocument5 pagesMedical Injuries or Illnesses To Use Medical Marijuana in ColoradoGreenpoint Insurance ColoradoNo ratings yet
- Alcohol and Drug Abuse Division (ADAD) Substance Use Disorder Treatment Rules Colorado DHSDocument80 pagesAlcohol and Drug Abuse Division (ADAD) Substance Use Disorder Treatment Rules Colorado DHSBrian HarrisNo ratings yet
- Colorado Guidelines of Professional Practice For Controlled SubstancesDocument65 pagesColorado Guidelines of Professional Practice For Controlled SubstancesBrian HarrisNo ratings yet
- The DEA Position On MarijuanaDocument63 pagesThe DEA Position On MarijuanaBrian HarrisNo ratings yet
- 42 CFR Part 8 Opioid Drugs in Maintenance and Detoxification Treatment of Opiate Addiction Final RuleDocument28 pages42 CFR Part 8 Opioid Drugs in Maintenance and Detoxification Treatment of Opiate Addiction Final RuleBrian HarrisNo ratings yet
- Pharmacist's Manual - An Information Outline of The Controlled Substances Act - 2010Document85 pagesPharmacist's Manual - An Information Outline of The Controlled Substances Act - 2010James LindonNo ratings yet
- Reparation, Characterization, and Optimization of Microemulsion For Topical Delivery of ItraconazoleDocument10 pagesReparation, Characterization, and Optimization of Microemulsion For Topical Delivery of ItraconazoleVeni UNNo ratings yet
- Lesson PlanDocument5 pagesLesson Planapi-456870847No ratings yet
- Camca Prelim Reviewer 2Document11 pagesCamca Prelim Reviewer 2Danna MedranaNo ratings yet
- NP 5Document6 pagesNP 5Ana Blesilda Cachola100% (1)
- Radiographic Positioning and Related Anatomy 8Th Edition Bontrager Test Bank Full Chapter PDFDocument35 pagesRadiographic Positioning and Related Anatomy 8Th Edition Bontrager Test Bank Full Chapter PDFdecagrambarrymfh100% (5)
- Shade Establishment and Management in Tea FieldsDocument55 pagesShade Establishment and Management in Tea Fieldschinthaka100% (1)
- Biological Classification BioHackDocument15 pagesBiological Classification BioHackAdhithyan M100% (2)
- Medical Mnemonics 4 PrintDocument65 pagesMedical Mnemonics 4 Printanne0521100% (1)
- AUTISM IN CHILDREN: SIGNS, ASSESSMENT AND INTERVENTIONDocument5 pagesAUTISM IN CHILDREN: SIGNS, ASSESSMENT AND INTERVENTIONvai2No ratings yet
- ArthropodaDocument36 pagesArthropodatapas kunduNo ratings yet
- YMMNO ProposalDocument2 pagesYMMNO ProposalYamon Min Nyunt OoNo ratings yet
- Noveon Laser ComparisonDocument20 pagesNoveon Laser ComparisonJohn KenneyNo ratings yet
- Standard LFT and It's Clinical SignificanceDocument28 pagesStandard LFT and It's Clinical SignificanceanimathzNo ratings yet
- Gene TherapyDocument10 pagesGene Therapyaaman sharmaNo ratings yet
- Mechanical Ventilation Handout - AllenhoDocument23 pagesMechanical Ventilation Handout - AllenhoCarmen HerediaNo ratings yet
- RH BLOOD GROUPDocument23 pagesRH BLOOD GROUPWho KnowsNo ratings yet
- Rabipur - (EMC) Print FriendlyDocument8 pagesRabipur - (EMC) Print Friendlyshreyas_chandor3802No ratings yet
- 3911515Document1 page3911515Gemmelle CangcoNo ratings yet
- Pathomechanisms of Common Gynecological Diseases in Chinese Medicine PDFDocument52 pagesPathomechanisms of Common Gynecological Diseases in Chinese Medicine PDFdc6463No ratings yet
- Understanding human factors in aviation safety and performanceDocument15 pagesUnderstanding human factors in aviation safety and performanceMoslem GrimaldiNo ratings yet
- Three Types of BiodiversityDocument3 pagesThree Types of BiodiversityMaruthi Nayaka J PNo ratings yet
- November 2, 2012 Strathmore TimesDocument32 pagesNovember 2, 2012 Strathmore TimesStrathmore TimesNo ratings yet
- Paediatric Examination Handbook 2015Document66 pagesPaediatric Examination Handbook 2015Ulfa Rahmadanti SetiawanNo ratings yet
- Wu2014 PDFDocument20 pagesWu2014 PDFmarioaNo ratings yet
- Reversing Chronic Diseases in Children PDFDocument10 pagesReversing Chronic Diseases in Children PDFFalk WendtNo ratings yet
- Bears and mice friendship in a storyDocument14 pagesBears and mice friendship in a storyKai PacNo ratings yet
- COPD Case StudyDocument4 pagesCOPD Case StudyPj Declarador100% (4)
- Generic Name: Brand Name: Apo-Metoprolol, Betaloc, Lopressor, Novo-Metoprolol, Nu-Drug ClassificationDocument4 pagesGeneric Name: Brand Name: Apo-Metoprolol, Betaloc, Lopressor, Novo-Metoprolol, Nu-Drug ClassificationKat ZNo ratings yet
- Digestive System and Respiratory SystemDocument10 pagesDigestive System and Respiratory SystemKathMae BoaNo ratings yet
- 1536106348Document144 pages1536106348Saman SarKoNo ratings yet