You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Mcqs CardiaologyDocument17 pagesMcqs CardiaologyMirza GhalibNo ratings yet
- Invitation Flyer MERGEDDocument2 pagesInvitation Flyer MERGEDzulmynurNo ratings yet
- Esc Guidelines 2020 Nste-Acs FinalDocument34 pagesEsc Guidelines 2020 Nste-Acs FinalabcdefNo ratings yet
- Ped CardioDocument18 pagesPed CardioIdioness100% (1)
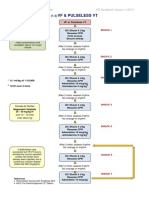
- VF & Pulseless VTDocument1 pageVF & Pulseless VTmadimadi11No ratings yet
- Ecg - Basics For The Anesthesiologists: Dr.K.M.LakshmanarajanDocument145 pagesEcg - Basics For The Anesthesiologists: Dr.K.M.LakshmanarajanKM Lakshmana RajanNo ratings yet
- Renal Exam Class TestDocument8 pagesRenal Exam Class Test1fleetingNo ratings yet
- Ecg Charts - PDF Final - Doc 2016Document6 pagesEcg Charts - PDF Final - Doc 2016ZweNo ratings yet
- Boxer Dog Cardiomyopathy: An Update: Kathryn M. Meurs, DVM, PHDDocument10 pagesBoxer Dog Cardiomyopathy: An Update: Kathryn M. Meurs, DVM, PHDOdrig De LavalleNo ratings yet
- European J of Heart Fail - 2022 - Bay S Gen S - Head To Head Comparison Between Recommendations by The ESC and ACC AHA HFSADocument11 pagesEuropean J of Heart Fail - 2022 - Bay S Gen S - Head To Head Comparison Between Recommendations by The ESC and ACC AHA HFSANora ArroyoNo ratings yet
- Hypertensive Emgerencies 2021Document19 pagesHypertensive Emgerencies 2021Faranitach AiniNo ratings yet
- EKG in IHDDocument349 pagesEKG in IHDDinhLinh100% (1)
- MCQ1Document11 pagesMCQ1Yuda Lutfiadi100% (1)
- Anatomy and PhysiologyDocument3 pagesAnatomy and PhysiologyChristopher bruncanoNo ratings yet
- The Role of BB in Hypertensive Patients With SODocument12 pagesThe Role of BB in Hypertensive Patients With SOjimNo ratings yet
- Ventricular Sense ResponseDocument3 pagesVentricular Sense ResponseDaniel Banina AguerreNo ratings yet
- ROLE OF STREPTOKINASE - OdpDocument7 pagesROLE OF STREPTOKINASE - OdpShumyle Mukhtar HussainNo ratings yet
- Rheumatic Heart DiseaseDocument3 pagesRheumatic Heart DiseaseWay LeeNo ratings yet
- Congenital Heart DiseaseDocument93 pagesCongenital Heart DiseaseManjunatha HR100% (1)
- Pathophysiology of Acute Kidney Injury (Aki) Caused by ShockDocument26 pagesPathophysiology of Acute Kidney Injury (Aki) Caused by ShockbokobokobokanNo ratings yet
- Full Programme 9 PDFDocument18 pagesFull Programme 9 PDFBorneo CTVSNo ratings yet
- QC CardiologistDocument10 pagesQC CardiologistJefferson VelonzaNo ratings yet
- CAD - Ischemic Heart Disease: AtherosclerosisDocument5 pagesCAD - Ischemic Heart Disease: Atherosclerosisbri ngNo ratings yet
- Cardiovascular Short Notes Review 1Document11 pagesCardiovascular Short Notes Review 1Jyothi100% (2)
- Robert G Gish CV October 2014Document228 pagesRobert G Gish CV October 2014Robert G. Gish, MDNo ratings yet
- PDF Rigel PatSim 200Document5 pagesPDF Rigel PatSim 200Eliel VelasquezNo ratings yet
- Echo Facts IndexDocument3 pagesEcho Facts Indexs336336anl100% (1)
- Cystatin C y Neutrophil Gelatinase-Associated Lipocalin Como Biomarcadores Tempranos para La Enfermedad Renal Crónica en PerrosDocument6 pagesCystatin C y Neutrophil Gelatinase-Associated Lipocalin Como Biomarcadores Tempranos para La Enfermedad Renal Crónica en PerrosventasNo ratings yet
- ECG Mastery Improving Your ECG Interpretation SkillsDocument23 pagesECG Mastery Improving Your ECG Interpretation SkillsHitesh Deora100% (2)
- Cardiology - Pericardial Disease PDFDocument1 pageCardiology - Pericardial Disease PDFPshtiwan MahmoodNo ratings yet