You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Cancer JournalDocument9 pagesCancer JournalRidha Surya NugrahaNo ratings yet
- Chronic Complications Diabetes - Acta Med Indones - Edit 8 Apr 14Document9 pagesChronic Complications Diabetes - Acta Med Indones - Edit 8 Apr 14Ridha Surya Nugraha100% (1)
- MindMapper Tutorial PDFDocument1 pageMindMapper Tutorial PDFRidha Surya NugrahaNo ratings yet
- Cancer Malignancy TumorDocument6 pagesCancer Malignancy TumorRidha Surya NugrahaNo ratings yet
- Cancer PathologyDocument7 pagesCancer PathologyRidha Surya NugrahaNo ratings yet
- Cancer InformationDocument6 pagesCancer InformationRidha Surya NugrahaNo ratings yet
- Cancer JournalDocument9 pagesCancer JournalRidha Surya NugrahaNo ratings yet
- Bangs atDocument1 pageBangs atRidha Surya NugrahaNo ratings yet
- Anemia Def FeDocument1 pageAnemia Def FeRidha Surya NugrahaNo ratings yet
- Basal Ganglia & Degenerative DisordersDocument46 pagesBasal Ganglia & Degenerative DisordersRidha Surya NugrahaNo ratings yet
- Noise - Induced Hejaring Loss. (DR - Khayria) - 2mlkmlkmDocument13 pagesNoise - Induced Hejaring Loss. (DR - Khayria) - 2mlkmlkmRidha Surya NugrahaNo ratings yet
- Link Donlot FilmDocument1 pageLink Donlot FilmRidha Surya NugrahaNo ratings yet
- Clinical of StrokeDocument31 pagesClinical of StrokeIlham riandaNo ratings yet
- Set Aaaaaaaaaaaa NNNDocument1 pageSet Aaaaaaaaaaaa NNNRidha Surya NugrahaNo ratings yet
- A A A AaaaaaaaaaaaaaaDocument1 pageA A A AaaaaaaaaaaaaaaRidha Surya NugrahaNo ratings yet
- 2008 SNAREmediated Membrane FusionDocument7 pages2008 SNAREmediated Membrane FusionRidha Surya NugrahaNo ratings yet
- 2008 Synaptic Vesicle FusionDocument10 pages2008 Synaptic Vesicle FusionRidha Surya NugrahaNo ratings yet
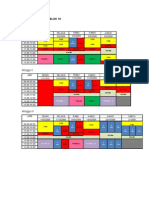
- Matriks Kegiatan Blok 10Document2 pagesMatriks Kegiatan Blok 10Ridha Surya NugrahaNo ratings yet
- 2007 TAG SynapticDocument5 pages2007 TAG SynapticRidha Surya NugrahaNo ratings yet
- RAV Nonproliferative Diabetic Retinopathy NPDRDocument1 pageRAV Nonproliferative Diabetic Retinopathy NPDRRidha Surya NugrahaNo ratings yet
- Original Article: Clinical and Laboratory Features of Typhoid Fever in ChildhoodDocument6 pagesOriginal Article: Clinical and Laboratory Features of Typhoid Fever in ChildhoodRidha Surya NugrahaNo ratings yet
- OijijlllllDocument1 pageOijijlllllRidha Surya NugrahaNo ratings yet
- RAV Nonproliferative Diabetic Retinopathy NPDRDocument1 pageRAV Nonproliferative Diabetic Retinopathy NPDRRidha Surya NugrahaNo ratings yet
- Sdasldmk MCDMFL DSFDocument1 pageSdasldmk MCDMFL DSFRidha Surya NugrahaNo ratings yet
- Speedy Instal at IonDocument1 pageSpeedy Instal at IonRidha Surya NugrahaNo ratings yet
- Daftar PustakaDocument1 pageDaftar PustakaRidha Surya NugrahaNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- ASV GalileoDocument43 pagesASV GalileoalvyandaniNo ratings yet
- A Review Paper On Scope of Big Data Analysis in Heath INFORMATICSDocument8 pagesA Review Paper On Scope of Big Data Analysis in Heath INFORMATICSMohamed Aly SowNo ratings yet
- Wa0003Document4 pagesWa0003YegaNo ratings yet
- ROLE OF DIAGNOSTIC LAPROSCOPY IN MANAGEMENT OF ACUTE Abdomen FinalDocument80 pagesROLE OF DIAGNOSTIC LAPROSCOPY IN MANAGEMENT OF ACUTE Abdomen Finalnaveena reddyNo ratings yet
- The Anatomy of BreathingDocument6 pagesThe Anatomy of BreathingmihaiylaNo ratings yet
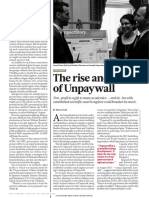
- Unpaywall ArticleDocument2 pagesUnpaywall ArticleChristian HdezNo ratings yet
- List COVID Facilities State OdishaDocument3 pagesList COVID Facilities State OdishadrjyotivetNo ratings yet
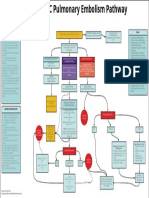
- EMCrit Lae Pulmonary FlowDocument1 pageEMCrit Lae Pulmonary FlowhmsptrNo ratings yet
- Elisa PPT Nitub 2019Document57 pagesElisa PPT Nitub 2019Nabila Bahar100% (1)
- Course Task 19Document1 pageCourse Task 19Laira CañeteNo ratings yet
- Cardiocare 2000 Operation ManualDocument61 pagesCardiocare 2000 Operation ManualDokter MoezNo ratings yet
- Beauty's Dirty SecretDocument188 pagesBeauty's Dirty SecretMarmotini100% (1)
- Plant Structures and Physiology NotesDocument97 pagesPlant Structures and Physiology Notesapi-292966101No ratings yet
- PathogenesisDocument14 pagesPathogenesisIdreesNo ratings yet
- Tomatoes and Tomato Products - Nutritional, Medicinal and Therapeutic PropertiesDocument664 pagesTomatoes and Tomato Products - Nutritional, Medicinal and Therapeutic PropertiesAndreea MerţNo ratings yet
- Effects of A Photochemical SmogDocument4 pagesEffects of A Photochemical SmogKumar RajNo ratings yet
- Physiology Study Guide CH 7 Nervous System Neurons KeyDocument4 pagesPhysiology Study Guide CH 7 Nervous System Neurons KeyJamie SamuelNo ratings yet
- Notice: Ocean Transportation Intermediary Licenses: InterCaribbean Cargo, Inc., Et Al.Document2 pagesNotice: Ocean Transportation Intermediary Licenses: InterCaribbean Cargo, Inc., Et Al.Justia.comNo ratings yet
- Chemistry Investigatory Project 2017-18Document29 pagesChemistry Investigatory Project 2017-18Ashok KumarNo ratings yet
- Inheritance and Selective Breeding QsDocument27 pagesInheritance and Selective Breeding QspartinpoutsamouNo ratings yet
- A Bad Case of StripesDocument2 pagesA Bad Case of StripesRadhika RathoreNo ratings yet
- Bee Empowerment Leslie WilsonDocument6 pagesBee Empowerment Leslie Wilsonchakravartys1327100% (1)
- 常用詞彙表Document10 pages常用詞彙表GXNo ratings yet
- Inles 4Document2 pagesInles 4Astrid CruzNo ratings yet
- Free Class Asclepio Metabolic SyndromeDocument6 pagesFree Class Asclepio Metabolic SyndromeJames BudiantoNo ratings yet
- Imaging of Intracranial InfectionsDocument12 pagesImaging of Intracranial Infectionsrafael rocha novaesNo ratings yet
- Guidelines On NADOPOD Regulations 2004Document28 pagesGuidelines On NADOPOD Regulations 2004LuqmanAlHakimNo ratings yet
- Chapter 22 Exile in DapitanDocument5 pagesChapter 22 Exile in DapitanJohn Terrence M. Romero83% (6)
- Hospital Environment For Sick ChildDocument10 pagesHospital Environment For Sick ChildKhushbu KatariaNo ratings yet
- Language and ArtsDocument17 pagesLanguage and ArtsOpium PoppyNo ratings yet