You might also like
- Neuroplasticity Social ExercisesDocument1 pageNeuroplasticity Social ExercisesginanimaNo ratings yet
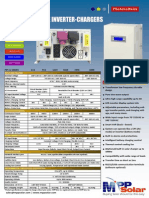
- Low Frequency Pure Sine Wave Solar Inverter ChargerDocument1 pageLow Frequency Pure Sine Wave Solar Inverter ChargerginanimaNo ratings yet
- First WeekDocument1 pageFirst WeekMichaelGeorgeNo ratings yet
- PSYCHOANALYTIC PERSONALITY ASSESSMENTDocument4 pagesPSYCHOANALYTIC PERSONALITY ASSESSMENTginanimaNo ratings yet
- First WeekDocument1 pageFirst WeekMichaelGeorgeNo ratings yet
- Universitatea Din Bucureşti: Facultatea de Psihologie Şi Ştiinţele EducaţieiDocument27 pagesUniversitatea Din Bucureşti: Facultatea de Psihologie Şi Ştiinţele Educaţieiginanima100% (4)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Psych Practice ExamDocument21 pagesPsych Practice Examstuffednurse100% (1)
- Disorder of Adult PersonalityDocument71 pagesDisorder of Adult Personalitychindy layNo ratings yet
- Gender Dysphoria & ADHDDocument21 pagesGender Dysphoria & ADHDAndrew StewartNo ratings yet
- Clinical - Assessment PTSD in Children With Mild To BorderlineDocument8 pagesClinical - Assessment PTSD in Children With Mild To BorderlineSyifa MunawarahNo ratings yet
- Childhood Trauma, Dissociation, and Psychiatric Comorbidity in Patients With Conversion DisorderDocument6 pagesChildhood Trauma, Dissociation, and Psychiatric Comorbidity in Patients With Conversion DisorderCarla MesquitaNo ratings yet
- Chapter 6: Somatoform and Dissociative DisordersDocument19 pagesChapter 6: Somatoform and Dissociative DisordersEsraRamos100% (1)
- Mental Status ExaminationDocument13 pagesMental Status ExaminationJosé Ramón Pérez-Accino100% (1)
- Keeping Your Balance - 01 - Overview of Bipolar DisorderDocument9 pagesKeeping Your Balance - 01 - Overview of Bipolar DisorderMarNo ratings yet
- Notes:: Time Allowed: Reading Time: 5 Minutes Writing Time: 40 MinutesDocument2 pagesNotes:: Time Allowed: Reading Time: 5 Minutes Writing Time: 40 Minutesmaimoona sulemanNo ratings yet
- Psychiatry Board Prep - Spiegel and Kenny - v3 - Tabbed PDFDocument1,083 pagesPsychiatry Board Prep - Spiegel and Kenny - v3 - Tabbed PDFBM L100% (1)
- Initial EvaluationDocument2 pagesInitial EvaluationStephan CarlsonNo ratings yet
- My Brother Tom's Schizophrenia: by Marin SardyDocument10 pagesMy Brother Tom's Schizophrenia: by Marin Sardyapi-450510068No ratings yet
- Modern Problem: Smartphone AddictionDocument3 pagesModern Problem: Smartphone Addictionstarryfacehao83% (6)
- Psychiatric Interview, MSEDocument48 pagesPsychiatric Interview, MSEComia Karla100% (1)
- Clinical Case Scenarios 2Document3 pagesClinical Case Scenarios 2Jei NacalabanNo ratings yet
- Drug Addiction and Drug AbuseDocument7 pagesDrug Addiction and Drug Abusejc_chopraNo ratings yet
- Understanding Suicide From Diagnosis To Personalized TreatmentDocument444 pagesUnderstanding Suicide From Diagnosis To Personalized Treatmentbianca_rtjNo ratings yet
- Chapter 9 Personality DisordersDocument35 pagesChapter 9 Personality DisordersJuhi NathNo ratings yet
- Disruptive Mood Dysregulation DisorderDocument13 pagesDisruptive Mood Dysregulation DisorderNyoman SuryaNo ratings yet
- Time For A Paradigm ShiftDocument6 pagesTime For A Paradigm ShiftDavid GarcíaNo ratings yet
- RestrainingDocument9 pagesRestrainingRavi PaulNo ratings yet
- The Nocebo Effect Overdiagnosis and Its CostsDocument278 pagesThe Nocebo Effect Overdiagnosis and Its CostsmariusNo ratings yet
- Mental Illness Case Analysis 1Document8 pagesMental Illness Case Analysis 1api-545354167No ratings yet
- Stalk Essay 2Document8 pagesStalk Essay 2api-284104099No ratings yet
- Eating Dis. CH 23 PPT Edited-1Document28 pagesEating Dis. CH 23 PPT Edited-1Nicole PerezNo ratings yet
- Depression Scale for Older AdultsDocument4 pagesDepression Scale for Older AdultsFernanda CpNo ratings yet
- Process RecordingDocument3 pagesProcess Recordingdyosa 433% (9)
- Necrophilia: A Presentation by Caitlin GrayDocument9 pagesNecrophilia: A Presentation by Caitlin GrayCat GrayNo ratings yet
- Beliefs and Experiences in Hoarding PDFDocument12 pagesBeliefs and Experiences in Hoarding PDFSara Tobón GrajalesNo ratings yet
- DSM 5 IntroDocument9 pagesDSM 5 IntroSURYANo ratings yet