You might also like
- Problem Statement ObjectivesDocument4 pagesProblem Statement ObjectivesAmanda Scarlet100% (2)
- A Study To Assess The Effectiveness of Information Booklet On Outcome of Teen Age Pregnancy in Terms of Knowledge of Adolescent Girls in Selected Higher Secondary Schools at SurendranagarDocument4 pagesA Study To Assess The Effectiveness of Information Booklet On Outcome of Teen Age Pregnancy in Terms of Knowledge of Adolescent Girls in Selected Higher Secondary Schools at Surendranagarpatel hNo ratings yet
- Nursing 12Document81 pagesNursing 12Amit Barve50% (2)
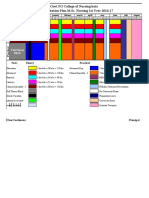
- 10.master Rotation Plan M. Sc. Nursing 1st YearDocument4 pages10.master Rotation Plan M. Sc. Nursing 1st YearNaresh JeengarNo ratings yet
- SNCDocument9 pagesSNCValarmathi100% (1)
- History and Development of Nursing ProfessionDocument22 pagesHistory and Development of Nursing Professionpriyanka50% (2)
- pdf2 PDFDocument125 pagespdf2 PDFsushma shresthaNo ratings yet
- Effectiveness of structured teaching programme on knowledge regarding effect of junk foodDocument156 pagesEffectiveness of structured teaching programme on knowledge regarding effect of junk foodCynthia Joy Ibhafidon100% (1)
- Annotated Bibliography of Advance Nursing PracticeDocument4 pagesAnnotated Bibliography of Advance Nursing PracticeKaku ManishaNo ratings yet
- Role of Inc SNC Boards and UniversitiesDocument70 pagesRole of Inc SNC Boards and UniversitiesSree LathaNo ratings yet
- Statement Problem NSGDocument64 pagesStatement Problem NSGarchna gargNo ratings yet
- Master of Philosophy Programme in NursingDocument17 pagesMaster of Philosophy Programme in NursingSanjay Kumar SanjuNo ratings yet
- Effectiveness of structured teaching on UTI knowledgeDocument56 pagesEffectiveness of structured teaching on UTI knowledgeAmit Pasi75% (4)
- Finalized Research TopicsDocument6 pagesFinalized Research TopicsKhirabdhi Tanaya SahuNo ratings yet
- Problem Statements PresentationDocument7 pagesProblem Statements PresentationAaliyaan KhanNo ratings yet
- Annotated Bibliography of Nursing Education:: 1. Elakkuvana Bhaskara Raj and Nima Bhaskar (2015), "A Textbook ofDocument4 pagesAnnotated Bibliography of Nursing Education:: 1. Elakkuvana Bhaskara Raj and Nima Bhaskar (2015), "A Textbook ofKaku Manisha100% (1)
- Year: 2003 Faculty: NURSING Subject: Obstetrics and Gynaecological NursingDocument7 pagesYear: 2003 Faculty: NURSING Subject: Obstetrics and Gynaecological NursingSajo Mareena75% (4)
- Bincy PDFDocument171 pagesBincy PDFapi-250591879No ratings yet
- Synopsis FormatDocument13 pagesSynopsis FormatYemane Fish83% (6)
- History of MSNDocument20 pagesHistory of MSNSyamVRNo ratings yet
- Handouts On Research Problem StatementDocument2 pagesHandouts On Research Problem Statementvarshasharma05100% (1)
- Review Article On Acharya TechDocument5 pagesReview Article On Acharya Techrahul yadavNo ratings yet
- Research ProjectDocument15 pagesResearch ProjectPravalika NatarajanNo ratings yet
- Post BSC I YearDocument3 pagesPost BSC I Yearkuruvagadda sagarNo ratings yet
- YearDocument95 pagesYearBasil KuriakoseNo ratings yet
- Rajiv Gandhi University of Health Sciences Bangalore, KarnatakaDocument23 pagesRajiv Gandhi University of Health Sciences Bangalore, KarnatakaAmit TamboliNo ratings yet
- HISTORICAL DEVELOPMENT IN CARDIOLOGYDocument3 pagesHISTORICAL DEVELOPMENT IN CARDIOLOGYneha_minnie100% (4)
- ROTATION PLAN M.Sc. 1sr YRDocument1 pageROTATION PLAN M.Sc. 1sr YRRuchika KaushalNo ratings yet
- Title Page: Title of The Article: "A Study To Assess The Effectiveness of Structured Teaching Programme OnDocument9 pagesTitle Page: Title of The Article: "A Study To Assess The Effectiveness of Structured Teaching Programme OnInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- FOURTH YEAR BSC NURSING Course Plan - For MergeDocument33 pagesFOURTH YEAR BSC NURSING Course Plan - For MergeBHUKYA USHARANI50% (2)
- Preparation of Organizational Chart of College and HospitalDocument46 pagesPreparation of Organizational Chart of College and HospitalJyothi RameshNo ratings yet
- Vancouver and Apa StyleDocument8 pagesVancouver and Apa StylePankaj Khatri100% (1)
- BSC Nursing II Year Sociology Course PlanDocument35 pagesBSC Nursing II Year Sociology Course Planramtenki sreelekha100% (6)
- A Descriptive Study To Assess The Level of Stress and Coping Strategies Adopted by 1st Year B.SC (N) StudentsDocument6 pagesA Descriptive Study To Assess The Level of Stress and Coping Strategies Adopted by 1st Year B.SC (N) StudentsAnonymous izrFWiQNo ratings yet
- New Problem StatementDocument2 pagesNew Problem Statementrenuka rathore100% (2)
- PEPTIC ULCER LESSON PLANDocument7 pagesPEPTIC ULCER LESSON PLANVeenasravanthiNo ratings yet
- A Descriptive Study To Assess The Knowledge and Practice Regarding Adverse Effects of Excessive Use of Mobile Phones Among Nursing Students of Selected Nursing College of BagalkotDocument8 pagesA Descriptive Study To Assess The Knowledge and Practice Regarding Adverse Effects of Excessive Use of Mobile Phones Among Nursing Students of Selected Nursing College of BagalkotAnonymous izrFWiQNo ratings yet
- Ethical and Cultural Issues in Medical Surgical Nursing PDFDocument2 pagesEthical and Cultural Issues in Medical Surgical Nursing PDFLara50% (8)
- Current Status of Health and Disease Burden in IndiaDocument23 pagesCurrent Status of Health and Disease Burden in IndiaKavi rajput100% (1)
- Nursing Seminar on Health Problems and Data CollectionDocument11 pagesNursing Seminar on Health Problems and Data CollectionLekshmi ManuNo ratings yet
- Critical Analysis of M.sc. Program of Teacher Education in IndiaDocument13 pagesCritical Analysis of M.sc. Program of Teacher Education in Indiakiran mahal76% (17)
- Independent Practice Issues and Independent Midwifery Nursing PRACTIONERDocument14 pagesIndependent Practice Issues and Independent Midwifery Nursing PRACTIONERKrini Tandel100% (4)
- Biologic and Psychosocial Dynamics in Disease CausationDocument35 pagesBiologic and Psychosocial Dynamics in Disease Causationlivelinami100% (4)
- Annotated Bibliography: College of Nursing Madurai Medical College, Madurai. A N PDocument6 pagesAnnotated Bibliography: College of Nursing Madurai Medical College, Madurai. A N PValarmathi100% (1)
- Development and Maintenance of Standards and Accreditation ofDocument38 pagesDevelopment and Maintenance of Standards and Accreditation ofsrimalathi100% (1)
- Annotated Bibliography of Research & StatisticsDocument4 pagesAnnotated Bibliography of Research & StatisticsKaku ManishaNo ratings yet
- ThesisDocument30 pagesThesisSimran JosanNo ratings yet
- Historical Development of Community Health and Community HealthDocument107 pagesHistorical Development of Community Health and Community HealthHarini100% (1)
- Futuristic Nursing TrendsDocument14 pagesFuturistic Nursing TrendsPhebeDimple100% (2)
- Group DynamicsDocument21 pagesGroup DynamicsPandiyan Dhyan100% (1)
- Major Stakeholders in Health Care SystemDocument5 pagesMajor Stakeholders in Health Care SystemANITTA S100% (1)
- Cultural & Ethical Nursing Care for Medical & Surgical PatientsDocument36 pagesCultural & Ethical Nursing Care for Medical & Surgical PatientsDHARAJIYA CHANDRIKA100% (8)
- Nursing Autonomy and AccountabilityDocument6 pagesNursing Autonomy and AccountabilityRabu75% (4)
- Effectiveness of Planned Teaching Programme On Knowledge of Emergency Drugs Among Staff NursesDocument4 pagesEffectiveness of Planned Teaching Programme On Knowledge of Emergency Drugs Among Staff NursesRumela Ganguly ChakrabortyNo ratings yet
- Health PromotionDocument127 pagesHealth PromotionThokala SujatjaNo ratings yet
- Defining levels of preventionDocument23 pagesDefining levels of preventionkuruvagadda sagar100% (1)
- Subject: Advanced Nursing Practice Topic: Treatment Aspects: Pharmacological and Pre and Post Operative Care AspectsDocument44 pagesSubject: Advanced Nursing Practice Topic: Treatment Aspects: Pharmacological and Pre and Post Operative Care Aspectsankita100% (1)
- Update on Osteoarthritis Burden and TreatmentDocument31 pagesUpdate on Osteoarthritis Burden and TreatmentZeeshan IslamNo ratings yet
- Epsom SaltDocument48 pagesEpsom SaltSathya Palanisamy100% (1)
- Arthritis and Society: The Impact of Musculoskeletal DiseasesFrom EverandArthritis and Society: The Impact of Musculoskeletal DiseasesNo ratings yet
- Soal Bahasa Inggris SNMPTN 2008 101Document5 pagesSoal Bahasa Inggris SNMPTN 2008 101DittoCendykiaIINo ratings yet
- Jurnal Noma PDFDocument7 pagesJurnal Noma PDFUtmi Arma DrgNo ratings yet
- A Case Report On Kartagener's SyndromeDocument3 pagesA Case Report On Kartagener's SyndromeBaru Chandrasekhar RaoNo ratings yet
- 18c. Lymphoma EditedDocument36 pages18c. Lymphoma EditedMUHAMMAD BAGIR ALJUFRINo ratings yet
- Imaging in Otosclerosis: A Pictorial ReviewDocument8 pagesImaging in Otosclerosis: A Pictorial ReviewChlo14No ratings yet
- Meat Processing HygieneDocument17 pagesMeat Processing HygieneJonyBlessing100% (1)
- Chap 6 TabaccoDocument4 pagesChap 6 TabaccoSabina MoolyeNo ratings yet
- Personal View: OnlineDocument9 pagesPersonal View: OnlineMaria YustinaNo ratings yet
- Hypnotic Suggestibility and Its NatureDocument21 pagesHypnotic Suggestibility and Its NatureRaluka RalucaNo ratings yet
- Bleeding Disorders: Coagulopathy (Also Called Clotting Disorder and Bleeding DisorderDocument5 pagesBleeding Disorders: Coagulopathy (Also Called Clotting Disorder and Bleeding DisorderAyisha EdwinNo ratings yet
- MEDICAL ABBREVIATIONS AND BLOOD KNOWLEDGEDocument12 pagesMEDICAL ABBREVIATIONS AND BLOOD KNOWLEDGEShania Kate Ledesma ManabatNo ratings yet
- Arterial Blood Gas (ABG) Analysis: Normal ValuesDocument3 pagesArterial Blood Gas (ABG) Analysis: Normal ValuesNayem Hossain HemuNo ratings yet
- Oncologic NursingDocument16 pagesOncologic NursingDharline Abbygale Garvida AgullanaNo ratings yet
- 16 Drugs Affecting RespiDocument3 pages16 Drugs Affecting RespiAdriwayne Francis GonzalesNo ratings yet
- Clinical Examination in Ophthalmology PDFDocument400 pagesClinical Examination in Ophthalmology PDFYashwanth Gowda100% (1)
- Asbestos Controls and RegulationsDocument66 pagesAsbestos Controls and RegulationsvdiazsuarezNo ratings yet
- Elder Abuse and Neglect: Brenda Holmes MSN/Ed, RNDocument25 pagesElder Abuse and Neglect: Brenda Holmes MSN/Ed, RNSonia SinghNo ratings yet
- Carmen Final Test L1 2011-2Document6 pagesCarmen Final Test L1 2011-2Rodrigo CarvalhoNo ratings yet
- Hemodynamic MonitoringDocument28 pagesHemodynamic MonitoringKimberlie Dela Merced Tomas100% (1)
- Sensory ExamDocument24 pagesSensory Examsarguss14100% (2)
- DM Final PDFDocument15 pagesDM Final PDFgiftyNo ratings yet
- Magnesium and Type 2 Diabetes: Mario Barbagallo, Ligia J DominguezDocument7 pagesMagnesium and Type 2 Diabetes: Mario Barbagallo, Ligia J DominguezbayuwinotoNo ratings yet
- Unit 2 Exercises GHIJKPDocument5 pagesUnit 2 Exercises GHIJKPAry OrtizNo ratings yet
- 3 ❤ Smart Sheet for History Taking in Pediatrics خلفية صفراءDocument14 pages3 ❤ Smart Sheet for History Taking in Pediatrics خلفية صفراءsalah almozahemNo ratings yet
- Çikmiş Sorularinin Luk Kismi: E-Yds 2020-13Document5 pagesÇikmiş Sorularinin Luk Kismi: E-Yds 2020-13Mustafa AriNo ratings yet
- Fact File Gastro Intestinal HormonesDocument2 pagesFact File Gastro Intestinal HormonesSudip DevadasNo ratings yet
- 84359Document5 pages84359Pedro Gouveia100% (1)
- Psych Case StudyDocument14 pagesPsych Case Studyapi-604581864No ratings yet
- UK Health Variations - Extra Case StudyDocument4 pagesUK Health Variations - Extra Case StudySashiNo ratings yet
- Day Care Centre: Benefits of Ambulatory SurgeryDocument17 pagesDay Care Centre: Benefits of Ambulatory SurgeryAnonymous ibmeej9No ratings yet