You might also like
- AYUSH AGARWAL Settlement LetterDocument5 pagesAYUSH AGARWAL Settlement LetterASHISH BANSALNo ratings yet
- HARSHUL JAIN Settlement LetterDocument5 pagesHARSHUL JAIN Settlement LetterASHISH BANSAL100% (1)
- MyReport AFBOP220091539 20220509165842Document1 pageMyReport AFBOP220091539 20220509165842rahul kumarNo ratings yet
- Medical Reimbursement (Supported by Bills) Hrms Application ParticularsDocument3 pagesMedical Reimbursement (Supported by Bills) Hrms Application ParticularsKarthikeyan GuruNo ratings yet
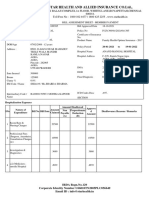
- Star Health and Allied Insurance Co - LTD.Document4 pagesStar Health and Allied Insurance Co - LTD.Parth MaradiyaNo ratings yet
- TR1703775325809 - 3 Pages - Vietnamese - RedactedDocument4 pagesTR1703775325809 - 3 Pages - Vietnamese - RedactedLyon HuynhNo ratings yet
- Sanskriti Agrwal Settlment LetterDocument5 pagesSanskriti Agrwal Settlment LetterASHISH BANSALNo ratings yet
- 29 Oqe PVMDocument5 pages29 Oqe PVMsharma7605No ratings yet
- Attachment MailDocument2 pagesAttachment MailQussai BitarNo ratings yet
- ReimbursementDocument1 pageReimbursementraviNo ratings yet
- Claim Settlement Letter 1688616797349Document6 pagesClaim Settlement Letter 1688616797349mailing.intern1No ratings yet
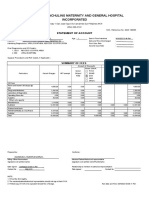
- Soa HospitalDocument1 pageSoa HospitalJocyl GonzagaNo ratings yet
- GAL CashlessEnhancementApprovalLetter CLMG 2022 131300 1510245 1645604895410Document6 pagesGAL CashlessEnhancementApprovalLetter CLMG 2022 131300 1510245 1645604895410Peter DarmalaNo ratings yet
- HDFC ERGO General Insurance Company LimitedDocument3 pagesHDFC ERGO General Insurance Company LimitedDhanush ChauhanNo ratings yet
- ApprovedDocument3 pagesApprovedajay jainNo ratings yet
- Backupnew PreAuthLetters ALIssuance 2022 SBIGI APR 28-04-2022-16-59-01 5456830Document2 pagesBackupnew PreAuthLetters ALIssuance 2022 SBIGI APR 28-04-2022-16-59-01 5456830MahanNo ratings yet
- Maxbupa Preauthorised Amount FinalDocument4 pagesMaxbupa Preauthorised Amount FinalraviNo ratings yet
- IRPF 2022 2021 Origi Imagem Declaracao01Document1 pageIRPF 2022 2021 Origi Imagem Declaracao01BVC RoleplayNo ratings yet
- Contributor Eligibility: Welcome HOS261Document3 pagesContributor Eligibility: Welcome HOS261Structural EngineerNo ratings yet
- GAL BillSummaryOtherProducts CLMG 2023 121316 0770148 1687159208225Document4 pagesGAL BillSummaryOtherProducts CLMG 2023 121316 0770148 1687159208225Sumathy GaneshNo ratings yet
- ApprovalLetterClaim LetterDocument4 pagesApprovalLetterClaim Lettersunny sohaniNo ratings yet
- Document PDFDocument2 pagesDocument PDFgregory binghamNo ratings yet
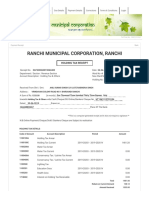
- Ranchi Municipal Corporation, Ranchi: Holding Tax ReceiptDocument2 pagesRanchi Municipal Corporation, Ranchi: Holding Tax ReceiptDurgesh Nandan Yadav0% (1)
- Del 1119 at 0001116Document4 pagesDel 1119 at 0001116waseemNo ratings yet
- Dr. P S Adhya 7186Document1 pageDr. P S Adhya 7186Partha AdhyaNo ratings yet
- PolicyScheduleDocument7 pagesPolicySchedulesrisaravananNo ratings yet
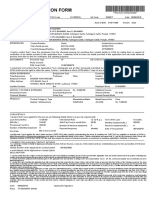
- Application Form: Applicant DetailsDocument1 pageApplication Form: Applicant DetailsPiyush PiyushNo ratings yet
- Tax Credit Certificate On Supplies: For General Tax Questions Call Our Toll Free 0800117000 or Log Onto URA Web PortalDocument1 pageTax Credit Certificate On Supplies: For General Tax Questions Call Our Toll Free 0800117000 or Log Onto URA Web Portalmawamajid2No ratings yet
- Claim Form Opd - To Be Filled in by The Insured: Details of Primary InsuredDocument2 pagesClaim Form Opd - To Be Filled in by The Insured: Details of Primary Insuredsumit1234ggNo ratings yet
- Paramount Health Services & Insurance Tpa Private Limited: Deficiency Letter Without PrejudiceDocument2 pagesParamount Health Services & Insurance Tpa Private Limited: Deficiency Letter Without PrejudiceHiren PanchalNo ratings yet
- Claim History StatementDocument2 pagesClaim History StatementFizza AliNo ratings yet
- Auto Credit Payment Notice: Philippine Health Insurance CorporationDocument1 pageAuto Credit Payment Notice: Philippine Health Insurance Corporationmahayag municipal hospitalNo ratings yet
- Preauth - 1-7Document2 pagesPreauth - 1-7SANTHOSH KUMARNo ratings yet
- Ericson Insurance Tpa Pvt. Limited.: Cashless Authorization Letter (Part-D)Document3 pagesEricson Insurance Tpa Pvt. Limited.: Cashless Authorization Letter (Part-D)baladon 007No ratings yet
- Session 1 - Final SettelmentDocument2 pagesSession 1 - Final SettelmentDipra DasNo ratings yet
- ClaimFormDocument9 pagesClaimFormVirat Vipul ChaudharyNo ratings yet
- Yadav Ji Medical FormDocument1 pageYadav Ji Medical FormRINL GZBNo ratings yet
- Shardaben N PatelDocument17 pagesShardaben N Patelniren4u1567No ratings yet
- Mediclaim FormatDocument3 pagesMediclaim Formatanand chawanNo ratings yet
- Policyholder Details: Certificate of InsuranceDocument5 pagesPolicyholder Details: Certificate of InsuranceSatyender ChouhanNo ratings yet
- Qou Shafiq HRPBDocument1 pageQou Shafiq HRPBNizzati NuhanNo ratings yet
- 27d89616-f058-4ed3-9ce0-07873a10d8a7Document2 pages27d89616-f058-4ed3-9ce0-07873a10d8a7Shri VigneshNo ratings yet
- E or Fee - Applied 20240112 618780100987 69100094Document1 pageE or Fee - Applied 20240112 618780100987 69100094riza.andal0928No ratings yet
- HMO Dependents Enrolment Form and Salary Deduction Authorization Form 20...Document1 pageHMO Dependents Enrolment Form and Salary Deduction Authorization Form 20...GemarieRoblesDelosReyesNo ratings yet
- Gur 0123 Pa 0003814 PDFDocument4 pagesGur 0123 Pa 0003814 PDFDdNo ratings yet
- Tax Invoice: Top-10 (Dahisar East)Document1 pageTax Invoice: Top-10 (Dahisar East)Aniket YadavNo ratings yet
- Job Offer-EXECUTIVE - ARDocument4 pagesJob Offer-EXECUTIVE - ARJ Nithin kumarNo ratings yet
- Recptno 236530520201124818Document1 pageRecptno 236530520201124818shorifmrhNo ratings yet
- MD Imran Final ApprovalDocument3 pagesMD Imran Final ApprovalASHISH BANSALNo ratings yet
- RoamDocument2 pagesRoamdivine mercyNo ratings yet
- ea7865d2-104b-4701-a854-83709d0baf97Document3 pagesea7865d2-104b-4701-a854-83709d0baf97chandru thanNo ratings yet
- GAL CashlessEnhancementApprovalLetter CLMG 2023 231214 1242860 1671785486860Document7 pagesGAL CashlessEnhancementApprovalLetter CLMG 2023 231214 1242860 1671785486860vikashNo ratings yet
- Cashless Authorization Letter (Part-D)Document6 pagesCashless Authorization Letter (Part-D)Kalyan.adaviNo ratings yet
- 1-10/1, MAIN ROAD Kommara, Attilli MD, W.G DT 534134 GSTIN/UIN: 37BLKPS4755C1ZS State Name: Andhra Pradesh, Code: 37Document1 page1-10/1, MAIN ROAD Kommara, Attilli MD, W.G DT 534134 GSTIN/UIN: 37BLKPS4755C1ZS State Name: Andhra Pradesh, Code: 37PraveenNo ratings yet
- Date: 07 Jul 2021 To,: (Please Quote This Reference Number in All Future Correspondence)Document2 pagesDate: 07 Jul 2021 To,: (Please Quote This Reference Number in All Future Correspondence)Manish SharmaNo ratings yet
- PSCS482553Document2 pagesPSCS482553Niran ChueachitNo ratings yet
- A Guide to District Court Civil Forms in the State of HawaiiFrom EverandA Guide to District Court Civil Forms in the State of HawaiiNo ratings yet
- Verilog GATE AND DATA FLOWDocument64 pagesVerilog GATE AND DATA FLOWPRIYA MISHRANo ratings yet
- Ep Docx Sca SMSC - V2Document45 pagesEp Docx Sca SMSC - V290007No ratings yet
- One and Half SindromeDocument4 pagesOne and Half SindromeYulia DamayantiNo ratings yet
- How Muslim Inventors Changed The WorldDocument4 pagesHow Muslim Inventors Changed The WorldShadab AnjumNo ratings yet
- Text Extraction From Image: Team Members CH - Suneetha (19mcmb22) Mohit Sharma (19mcmb13)Document20 pagesText Extraction From Image: Team Members CH - Suneetha (19mcmb22) Mohit Sharma (19mcmb13)suneethaNo ratings yet
- April 8/91: All GroupsDocument33 pagesApril 8/91: All Groupsreza mirzakhaniNo ratings yet
- History of Old English GrammarDocument9 pagesHistory of Old English GrammarAla CzerwinskaNo ratings yet
- PixiiDocument3 pagesPixiiFoxNo ratings yet
- Chemistry II EM Basic Learning MaterialDocument40 pagesChemistry II EM Basic Learning MaterialMAHINDRA BALLANo ratings yet
- PP Checklist (From IB)Document2 pagesPP Checklist (From IB)Pete GoodmanNo ratings yet
- Ericsson For Sale From Powerstorm 4SA03071242Document8 pagesEricsson For Sale From Powerstorm 4SA03071242wd3esaNo ratings yet
- Fall 3050 SyllabusDocument6 pagesFall 3050 Syllabustaher91No ratings yet
- Assesment Test in English 9Document3 pagesAssesment Test in English 9Chazz SatoNo ratings yet
- Invoice ApprovalDocument54 pagesInvoice ApprovalHamada Asmr AladhamNo ratings yet
- SQLDocument13 pagesSQLRadhakrishnan__7263No ratings yet
- Paper 4 Material Management Question BankDocument3 pagesPaper 4 Material Management Question BankDr. Rakshit Solanki100% (2)
- Translations Telugu To English A ClassifDocument111 pagesTranslations Telugu To English A ClassifGummadi Vijaya KumarNo ratings yet
- Case Study in Architectural Structures: A-7E Avionics System - ADocument36 pagesCase Study in Architectural Structures: A-7E Avionics System - Ajckz8No ratings yet
- Categories of Cargo and Types of ShipsDocument14 pagesCategories of Cargo and Types of ShipsVibhav Kumar100% (1)
- Mahindra First Choice Wheels LTD: 4-Wheeler Inspection ReportDocument5 pagesMahindra First Choice Wheels LTD: 4-Wheeler Inspection ReportRavi LoveNo ratings yet
- Teal Motor Co. Vs CFIDocument6 pagesTeal Motor Co. Vs CFIJL A H-DimaculanganNo ratings yet
- Credit CardDocument6 pagesCredit CardJ Boy LipayonNo ratings yet
- Chandigarh Distilers N BotlersDocument3 pagesChandigarh Distilers N BotlersNipun GargNo ratings yet
- M.Sc. Steel Structures LEC. #7 Plastic Analysis and Design: Dr. Qasim Shaukat KhanDocument43 pagesM.Sc. Steel Structures LEC. #7 Plastic Analysis and Design: Dr. Qasim Shaukat KhanSSNo ratings yet
- Synchronous Machines-1Document41 pagesSynchronous Machines-1Rouxcel abutoNo ratings yet
- Merging Shapes - 10 Minutes To Better Painting - Episode 1Document12 pagesMerging Shapes - 10 Minutes To Better Painting - Episode 1Nguyên HàNo ratings yet
- Limestone Standards PDFDocument2 pagesLimestone Standards PDFJacqueline BerueteNo ratings yet
- Master Data FileDocument58 pagesMaster Data Fileinfo.glcom5161No ratings yet
- FM Testbank-Ch18Document9 pagesFM Testbank-Ch18David LarryNo ratings yet
- Visual Inspection ReportDocument45 pagesVisual Inspection ReportKhoirul AnamNo ratings yet