You might also like
- Complications With The Power of LaborDocument8 pagesComplications With The Power of LaborEdrea Aquino MendezNo ratings yet
- Obstructed Labor-Bandl's RingDocument43 pagesObstructed Labor-Bandl's RingJune DumdumayaNo ratings yet
- Uterine RuptureDocument19 pagesUterine RuptureAna Denise Quinajon0% (1)
- Milestones of Fetal Growth and Development EssayDocument2 pagesMilestones of Fetal Growth and Development EssayZoe Dominique GudioNo ratings yet
- Esarean Ction: Cadalin, Fremelen Rose Cedamon, CarloDocument18 pagesEsarean Ction: Cadalin, Fremelen Rose Cedamon, CarloMonette Abalos MendovaNo ratings yet
- School of Health and Allied Health Sciences Nursing Department Self-Directed Learning (Nur 146 - Clinical Area)Document3 pagesSchool of Health and Allied Health Sciences Nursing Department Self-Directed Learning (Nur 146 - Clinical Area)Milagros FloritaNo ratings yet
- Caesarian: Saint John Colleges Calamba, City College of NursingDocument37 pagesCaesarian: Saint John Colleges Calamba, City College of NursingaudreylineNo ratings yet
- Ob MaternityDocument46 pagesOb MaternityJohanna Erazo Padilla100% (1)
- Precipitate Labor, Uterine Inversion, Uterine RuptureDocument3 pagesPrecipitate Labor, Uterine Inversion, Uterine RuptureAbbeygale Galan100% (2)
- Intrapartum Nursing Care GuideDocument78 pagesIntrapartum Nursing Care GuideKohinoorKohinoorNo ratings yet
- Intrapartal - Theories of LaborDocument21 pagesIntrapartal - Theories of LaborJan Oliver YaresNo ratings yet
- MCN Exam 2 Study Guide - CompleteDocument87 pagesMCN Exam 2 Study Guide - CompleteColin MacKenzie100% (1)
- Pa Tho Physiology of Uterine MyomaDocument2 pagesPa Tho Physiology of Uterine Myomaghettodawg187100% (7)
- LansoprazoleDocument3 pagesLansoprazoleJody FelizioNo ratings yet
- NSDDocument44 pagesNSDabyssodeep100% (1)
- Nursing Care of Postpartum ComplicationsDocument13 pagesNursing Care of Postpartum ComplicationsLyca Mae AurelioNo ratings yet
- Paracetamol Biogesic Analgesic AntipyreticDocument8 pagesParacetamol Biogesic Analgesic AntipyreticGian Era100% (1)
- SDL 3 MCN 1Document3 pagesSDL 3 MCN 1Milagros Florita100% (1)
- DystociaDocument31 pagesDystociamarsan120% (1)
- Methylergonovine maleate postpartum careDocument2 pagesMethylergonovine maleate postpartum careRitamariaNo ratings yet
- Forcep Delivery..Document3 pagesForcep Delivery..Kristelle Joy Capili SicatNo ratings yet
- Drugs StudyDocument6 pagesDrugs StudyMark_Rebibis_8528No ratings yet
- Sulfamethoxazole-trimethoprim drug cardDocument1 pageSulfamethoxazole-trimethoprim drug carderica2323No ratings yet
- What Are The Functions of Informed ConsentDocument2 pagesWhat Are The Functions of Informed ConsentKyla Angeli InfantadoNo ratings yet
- Ectopic Pregnancy - PathophysiologyDocument1 pageEctopic Pregnancy - PathophysiologyMarimiel PagulayanNo ratings yet
- Abruptio PlacentaDocument11 pagesAbruptio PlacentaAlynna ValbuenaNo ratings yet
- CefuroximeDocument11 pagesCefuroximeAlmira Ballesteros CestonaNo ratings yet
- Postpartum Complications 2015Document52 pagesPostpartum Complications 2015Janella Asis100% (1)
- Fetal Distress Causes and SymptomsDocument41 pagesFetal Distress Causes and Symptomsmarco luenaNo ratings yet
- Drug Study DRDocument6 pagesDrug Study DRBheigh Lomitao AlbueraNo ratings yet
- RLE 109 Group 4 Case Analysis in MastitisDocument20 pagesRLE 109 Group 4 Case Analysis in MastitisEugene MananganNo ratings yet
- Uterine AtonyDocument33 pagesUterine AtonyNonie 'Erni' HastiriniNo ratings yet
- Nursing Care PlanDocument7 pagesNursing Care Planrockerespi1283No ratings yet
- Ectopic PregnancyDocument26 pagesEctopic PregnancyCHryz TinNo ratings yet
- Case Study CS 3Document38 pagesCase Study CS 3tristanpaulNo ratings yet
- Normal Spontaneous DeliveryDocument64 pagesNormal Spontaneous DeliveryMichellin Andres MarianoNo ratings yet
- Drug Study FDocument3 pagesDrug Study FFatima Love Ariate-ArcasetasNo ratings yet
- Abruptio PlacentaDocument4 pagesAbruptio PlacentaChelzie LasernaNo ratings yet
- Labetalol Card#8Document1 pageLabetalol Card#8USMCDOC100% (1)
- OB Exam Nursing Care Labor DeliveryDocument2 pagesOB Exam Nursing Care Labor DeliveryLeah ElizabethNo ratings yet
- Drug StudyDocument3 pagesDrug Studybkr_wltr100% (2)
- Midterm Notes On NCM 109 EditedDocument10 pagesMidterm Notes On NCM 109 EditedJohn Fred100% (2)
- #3 Cesarean SectionDocument20 pages#3 Cesarean SectionDunice Lloyd Mata100% (1)
- What Is Bilateral Tubal LigationDocument42 pagesWhat Is Bilateral Tubal LigationAldrich ArquizaNo ratings yet
- Cs - Cesarean SectionDocument19 pagesCs - Cesarean Sectiondaph-me75% (16)
- The Four Stages of LaborDocument12 pagesThe Four Stages of LaborEdrea Aquino MendezNo ratings yet
- Problems With The PassagewayDocument43 pagesProblems With The PassagewayMathew Beniga Gaco92% (12)
- Difficult Labor (Dystocia) : Disproportion Between The Presenting Part of The Fetus and The Birth CanalDocument9 pagesDifficult Labor (Dystocia) : Disproportion Between The Presenting Part of The Fetus and The Birth CanalMohammad Hadi AlghuraifiNo ratings yet
- Abnormal Uterine Actions in ObstetricsDocument6 pagesAbnormal Uterine Actions in ObstetricsGhada SaadNo ratings yet
- Obstracted LabourDocument42 pagesObstracted LabourOmar mohamedNo ratings yet
- Passageway and Power Lesson 2: Problems With The PassagewayDocument3 pagesPassageway and Power Lesson 2: Problems With The PassagewayFatmah Sarah CornellNo ratings yet
- Intrapartum PeriodDocument19 pagesIntrapartum Periodanon_915924422No ratings yet
- Abnormal Uterine Contractions: Causes, Types & ManagementDocument68 pagesAbnormal Uterine Contractions: Causes, Types & ManagementDrPreeti Thakur ChouhanNo ratings yet
- DR Write UpDocument29 pagesDR Write UpmaryprincessuyNo ratings yet
- Prolonged pregnancy & abnormal uterine actionDocument110 pagesProlonged pregnancy & abnormal uterine actionAnnapurna DangetiNo ratings yet
- Obstetric & Gynecology Nursing: Topic-Physiological Changes During LabourDocument54 pagesObstetric & Gynecology Nursing: Topic-Physiological Changes During LabourBhumi ChouhanNo ratings yet
- ObDocument14 pagesObyayitsnayNo ratings yet
- Hands Out 3 LaborDocument29 pagesHands Out 3 LaborErin SaavedraNo ratings yet
- Cord Presentation ProlapseDocument10 pagesCord Presentation ProlapseJHONESSA LAYOSNo ratings yet
- Abnormal Uterine Action GuideDocument27 pagesAbnormal Uterine Action Guidetanmai noolu100% (1)
- The IntegumentDocument17 pagesThe IntegumentAnaNo ratings yet
- Competence Appraisal Cesarean SectionDocument20 pagesCompetence Appraisal Cesarean SectionAnaNo ratings yet
- The IntegumentDocument1 pageThe IntegumentAnaNo ratings yet
- Placenta Accreta ReportDocument13 pagesPlacenta Accreta ReportAnaNo ratings yet
- Soc Sci ReportDocument69 pagesSoc Sci ReportAnaNo ratings yet
- Soapie, Assessment and NCP On PAINDocument7 pagesSoapie, Assessment and NCP On PAINAna100% (2)
- Chest PhysiotherapyDocument5 pagesChest PhysiotherapyAnaNo ratings yet
- Competence Appraisal Cesarean SectionDocument20 pagesCompetence Appraisal Cesarean SectionAnaNo ratings yet
- Beliefs and Material Culture in The PhilippinesDocument4 pagesBeliefs and Material Culture in The PhilippinesAnaNo ratings yet
- A Case Study On Typhoid FeverDocument42 pagesA Case Study On Typhoid FeverAna92% (13)
- AntiPsychotic Drugs ReportDocument56 pagesAntiPsychotic Drugs ReportAnaNo ratings yet
- Stroke (Bisaya and English)Document4 pagesStroke (Bisaya and English)AnaNo ratings yet
- Retraction Ring LeafletDocument2 pagesRetraction Ring LeafletAna100% (1)
- Abnormal Progress in Labor (Precipitous Labor and Birth & Retraction Rings)Document34 pagesAbnormal Progress in Labor (Precipitous Labor and Birth & Retraction Rings)Ana100% (3)
- Uterine AnomaliesDocument24 pagesUterine AnomaliesAnaNo ratings yet
- DM-Health Teaching PlanDocument9 pagesDM-Health Teaching PlanAna86% (7)
- Different Substance Abuse and Their Effects To Pregnancy and FetusDocument5 pagesDifferent Substance Abuse and Their Effects To Pregnancy and FetusAnaNo ratings yet
- Immune System 2Document39 pagesImmune System 2AnaNo ratings yet
- FNCPDocument9 pagesFNCPAna100% (4)
- Assignment in NutritionDocument12 pagesAssignment in NutritionAnaNo ratings yet
- Immune SystemDocument58 pagesImmune SystemAnaNo ratings yet
- SporotrichosisDocument5 pagesSporotrichosisAna100% (1)
- Immunization SchedulesDocument3 pagesImmunization SchedulesAnaNo ratings yet
- CVA-Health Teaching PlanDocument5 pagesCVA-Health Teaching PlanAna100% (4)
- Prokaryotic & Eukaryotic Cells - 3Document47 pagesProkaryotic & Eukaryotic Cells - 3AnaNo ratings yet
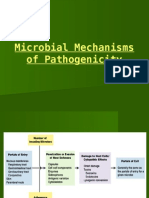
- Microbial Mechanisms of PathogenicityDocument29 pagesMicrobial Mechanisms of PathogenicityAnaNo ratings yet
- Microbial Diseases of The Skin & EyesDocument52 pagesMicrobial Diseases of The Skin & EyesAna100% (3)
- Microbial Diseases of The Respiratory SystemDocument9 pagesMicrobial Diseases of The Respiratory SystemAnaNo ratings yet
- Nursery Rhyme ActivitiesDocument13 pagesNursery Rhyme ActivitiesAnaNo ratings yet
- Water Cycle Cer 002Document2 pagesWater Cycle Cer 002api-434008934No ratings yet
- Minimizing Penalty in Industrialpower Factor Correction by Engaging Apfc UnitDocument15 pagesMinimizing Penalty in Industrialpower Factor Correction by Engaging Apfc UnitabellNo ratings yet
- Internal II BEEE QPDocument1 pageInternal II BEEE QPsivaNo ratings yet
- Chords ListDocument5 pagesChords ListakshayNo ratings yet
- Indian MaDocument1 pageIndian MaAnass LyamaniNo ratings yet
- Provisional RestorationsDocument9 pagesProvisional RestorationsshivaprasadmNo ratings yet
- Bushings BrochureDocument14 pagesBushings Brochurebpd21No ratings yet
- Manifest Guide Ebook PDFDocument4 pagesManifest Guide Ebook PDFAnonymous dqCHWEADzNo ratings yet
- Noun Form Answers PDFDocument11 pagesNoun Form Answers PDFChinna LingamNo ratings yet
- Deltopectoral Approach to the ShoulderDocument28 pagesDeltopectoral Approach to the ShoulderChrysi TsiouriNo ratings yet
- String TheoryDocument12 pagesString TheoryYashvinder SinghNo ratings yet
- Read Online Here: Bronto Skylift F32Document3 pagesRead Online Here: Bronto Skylift F32Randu WatangNo ratings yet
- Public List Programs by Specialty 460Document9 pagesPublic List Programs by Specialty 460Enta SyngNo ratings yet
- Table Napkin Folding TechniquesDocument6 pagesTable Napkin Folding TechniquesMiguel BaricuatroNo ratings yet
- Liugong 938l Wheel Loader Parts ManualDocument20 pagesLiugong 938l Wheel Loader Parts Manualviolet100% (56)
- Jyotish - A Manual of Hindu Astrology - B.v.raman - 1992Document149 pagesJyotish - A Manual of Hindu Astrology - B.v.raman - 1992Ram RamNo ratings yet
- The Concept of Representation in Psychology: January 1995Document11 pagesThe Concept of Representation in Psychology: January 1995laith AtekNo ratings yet
- Occupation Certificate DocumentsDocument1 pageOccupation Certificate Documentsarungupta366No ratings yet
- Ece-Research Work 1Document10 pagesEce-Research Work 1Peale ObiedoNo ratings yet
- Cology MCQDocument4 pagesCology MCQHemant BaraiNo ratings yet
- CKB 20104 Reaction Engineering UniKL MICET Experiment 1a: The Batch Saponification of Ethyl Acetate Full Lab ReportDocument11 pagesCKB 20104 Reaction Engineering UniKL MICET Experiment 1a: The Batch Saponification of Ethyl Acetate Full Lab ReportSiti Hajar Mohamed82% (11)
- ASME B36.10M-2004 Welded and Seamless Wrought Steel Pipe StandardDocument2 pagesASME B36.10M-2004 Welded and Seamless Wrought Steel Pipe StandardAmit BansalNo ratings yet
- Economic Growth, Environment and SustainabilityDocument3 pagesEconomic Growth, Environment and Sustainability140 - MANEESHA ST AGNESNo ratings yet
- Amplifiers and OscillatorsDocument109 pagesAmplifiers and OscillatorsAdilNo ratings yet
- Printing MachineDocument2 pagesPrinting MachinephamdoanketNo ratings yet
- Real-Time Reservoir Operation For Irrigation: P. P. Mujumdar and T. S. V. RameshDocument8 pagesReal-Time Reservoir Operation For Irrigation: P. P. Mujumdar and T. S. V. RameshGetachew BekeleNo ratings yet
- Angles of Elevation and Depression, Bearings NotesDocument4 pagesAngles of Elevation and Depression, Bearings Notesroddyeal100% (2)
- Thesis Defence Public Presentation FinalDocument16 pagesThesis Defence Public Presentation FinalAlina AndreevNo ratings yet
- Graphing linear functions and writing equations in standard formDocument15 pagesGraphing linear functions and writing equations in standard formnmarjonoNo ratings yet
- HYBRIFLEX® RRH Hybrid Cable Solution 12 X 24, 6AWG, Low-Inductance, Single-Mode Fiber, DLC Connectors Top and Bottom, 240 FTDocument3 pagesHYBRIFLEX® RRH Hybrid Cable Solution 12 X 24, 6AWG, Low-Inductance, Single-Mode Fiber, DLC Connectors Top and Bottom, 240 FTNoame Pauline SimbajonNo ratings yet
- Healing PCOS: A 21-Day Plan for Reclaiming Your Health and Life with Polycystic Ovary SyndromeFrom EverandHealing PCOS: A 21-Day Plan for Reclaiming Your Health and Life with Polycystic Ovary SyndromeNo ratings yet
- What to Expect When You’re Expecting (5th Edition)From EverandWhat to Expect When You’re Expecting (5th Edition)Rating: 5 out of 5 stars5/5 (1)
- The Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeFrom EverandThe Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeRating: 3.5 out of 5 stars3.5/5 (13)
- What No One Tells You: A Guide to Your Emotions from Pregnancy to MotherhoodFrom EverandWhat No One Tells You: A Guide to Your Emotions from Pregnancy to MotherhoodRating: 4.5 out of 5 stars4.5/5 (30)
- The Menopause Manifesto: Own Your Health With Facts and FeminismFrom EverandThe Menopause Manifesto: Own Your Health With Facts and FeminismRating: 4 out of 5 stars4/5 (18)
- Period Power: Harness Your Hormones and Get Your Cycle Working For YouFrom EverandPeriod Power: Harness Your Hormones and Get Your Cycle Working For YouRating: 4 out of 5 stars4/5 (25)
- All in Her Head: The Truth and Lies Early Medicine Taught Us About Women’s Bodies and Why It Matters TodayFrom EverandAll in Her Head: The Truth and Lies Early Medicine Taught Us About Women’s Bodies and Why It Matters TodayRating: 5 out of 5 stars5/5 (2)
- The Pain Gap: How Sexism and Racism in Healthcare Kill WomenFrom EverandThe Pain Gap: How Sexism and Racism in Healthcare Kill WomenRating: 4 out of 5 stars4/5 (153)
- ADHD Women: A Holistic Approach To ADHD ManagementFrom EverandADHD Women: A Holistic Approach To ADHD ManagementRating: 5 out of 5 stars5/5 (4)
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisFrom EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisRating: 3 out of 5 stars3/5 (2)
- Brain Body Diet: 40 Days to a Lean, Calm, Energized, and Happy SelfFrom EverandBrain Body Diet: 40 Days to a Lean, Calm, Energized, and Happy SelfRating: 5 out of 5 stars5/5 (2)
- The Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouFrom EverandThe Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouNo ratings yet
- Younger Next Year, 2nd Edition: Live Strong, Fit, Sexy, and Smart-Until You're 80 and BeyondFrom EverandYounger Next Year, 2nd Edition: Live Strong, Fit, Sexy, and Smart-Until You're 80 and BeyondRating: 4 out of 5 stars4/5 (110)
- Breaking Free from Body Shame: Dare to Reclaim What God Has Named GoodFrom EverandBreaking Free from Body Shame: Dare to Reclaim What God Has Named GoodRating: 5 out of 5 stars5/5 (33)
- I'm So Effing Tired: A Proven Plan to Beat Burnout, Boost Your Energy, and Reclaim Your LifeFrom EverandI'm So Effing Tired: A Proven Plan to Beat Burnout, Boost Your Energy, and Reclaim Your LifeRating: 4 out of 5 stars4/5 (15)
- The Path of the Priestess: A Guidebook for Awakening the Divine FeminineFrom EverandThe Path of the Priestess: A Guidebook for Awakening the Divine FeminineRating: 4 out of 5 stars4/5 (2)
- Not a Diet Book: Take Control. Gain Confidence. Change Your Life.From EverandNot a Diet Book: Take Control. Gain Confidence. Change Your Life.Rating: 4.5 out of 5 stars4.5/5 (124)
- The Hormone Secret: Discover Effortless Weight Loss and Renewed Energy in Just 30 DaysFrom EverandThe Hormone Secret: Discover Effortless Weight Loss and Renewed Energy in Just 30 DaysRating: 4.5 out of 5 stars4.5/5 (5)
- The First Forty Days: The Essential Art of Nourishing the New MotherFrom EverandThe First Forty Days: The Essential Art of Nourishing the New MotherRating: 5 out of 5 stars5/5 (5)
- A Radical Guide for Women with ADHD: Embrace Neurodiversity, Live Boldly, and Break Through BarriersFrom EverandA Radical Guide for Women with ADHD: Embrace Neurodiversity, Live Boldly, and Break Through BarriersRating: 4.5 out of 5 stars4.5/5 (71)
- Bumpin': The Modern Guide to Pregnancy: Navigating the Wild, Weird, and Wonderful Journey From Conception Through Birth and BeyondFrom EverandBumpin': The Modern Guide to Pregnancy: Navigating the Wild, Weird, and Wonderful Journey From Conception Through Birth and BeyondRating: 4.5 out of 5 stars4.5/5 (38)
- Women, Food, And Hormones: A 4-Week Plan to Achieve Hormonal Balance, Lose Weight, and Feel Like Yourself AgainFrom EverandWomen, Food, And Hormones: A 4-Week Plan to Achieve Hormonal Balance, Lose Weight, and Feel Like Yourself AgainRating: 4 out of 5 stars4/5 (14)
- The Mama Natural Week-by-Week Guide to Pregnancy and ChildbirthFrom EverandThe Mama Natural Week-by-Week Guide to Pregnancy and ChildbirthRating: 4.5 out of 5 stars4.5/5 (21)
- Stopping Stress Before It Stops You: A Game Plan for Every MomFrom EverandStopping Stress Before It Stops You: A Game Plan for Every MomRating: 4.5 out of 5 stars4.5/5 (20)
- 9 Months Is Not Enough: The Ultimate Pre-Pregnancy Checklist to Create a Baby-Ready Body and Build Generational HealthFrom Everand9 Months Is Not Enough: The Ultimate Pre-Pregnancy Checklist to Create a Baby-Ready Body and Build Generational HealthNo ratings yet
- The Better Period Food Solution: Eat Your Way to a Lifetime of Healthier CyclesFrom EverandThe Better Period Food Solution: Eat Your Way to a Lifetime of Healthier CyclesNo ratings yet