You might also like
- Cultural FinalDocument5 pagesCultural Finalapi-280998981No ratings yet
- Clinical Exemplar-1Document3 pagesClinical Exemplar-1api-280998981No ratings yet
- Discharge Planning ProjectDocument6 pagesDischarge Planning Projectapi-280998981No ratings yet
- Nursing Application EssayDocument2 pagesNursing Application Essayapi-280998981No ratings yet
- Medication SafetyDocument6 pagesMedication Safetyapi-280998981No ratings yet
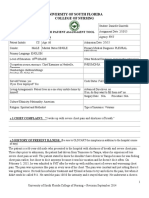
- Patient Assessment Tool ms2Document27 pagesPatient Assessment Tool ms2api-280998981No ratings yet
- Emory Cover Letter1Document1 pageEmory Cover Letter1api-280998981No ratings yet
- Patient Assessment Tool ms1Document27 pagesPatient Assessment Tool ms1api-280998981No ratings yet
- Patient Assessment Tool FundamentalsDocument22 pagesPatient Assessment Tool Fundamentalsapi-280998981No ratings yet
- Danielle Teresa GiaritelliDocument3 pagesDanielle Teresa Giaritelliapi-280998981No ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Andrew Haywood CV 2010Document6 pagesAndrew Haywood CV 2010Dobber0No ratings yet
- Arts & Science: Government First Grade College, AlavandiDocument5 pagesArts & Science: Government First Grade College, AlavandiAnonymous cyZVcDeNo ratings yet
- Transport Modelling Guidelines Volume 5 Intersection Modelling June 2020Document198 pagesTransport Modelling Guidelines Volume 5 Intersection Modelling June 2020Amul ShresthaNo ratings yet
- Fast Ai PDFDocument11 pagesFast Ai PDFfolioxNo ratings yet
- Catalogo Molas PratoDocument176 pagesCatalogo Molas Pratocassio_tecdrawNo ratings yet
- DistillationDocument8 pagesDistillationsahil khandelwalNo ratings yet
- ReportDocument39 pagesReportabi patowaryNo ratings yet
- The Peripatetic Observer 2003Document10 pagesThe Peripatetic Observer 2003SUNY Geneseo Department of EnglishNo ratings yet
- The Role of Youth in ForthDocument17 pagesThe Role of Youth in ForthSamuel EmmanuelNo ratings yet
- SB - New Worlds An Introduction To College Reading 5th EdDocument692 pagesSB - New Worlds An Introduction To College Reading 5th EdViệt HàNo ratings yet
- Psionic Bestiary - Phrenic HegemonyDocument12 pagesPsionic Bestiary - Phrenic HegemonyEduardo Ferreira SuzartNo ratings yet
- Siddique, Tashfeen Coverletter 20170320Document1 pageSiddique, Tashfeen Coverletter 20170320Anonymous liUNtnyNo ratings yet
- Discrete Mathematics Sets Relations FunctionsDocument15 pagesDiscrete Mathematics Sets Relations FunctionsMuhd FarisNo ratings yet
- Computer Keyboard Shortcut Keys PDFDocument7 pagesComputer Keyboard Shortcut Keys PDFmuhammad sohail janjuaNo ratings yet
- EVMDocument4 pagesEVMSimNo ratings yet
- S6a S13 GX RX InterfacesDocument4 pagesS6a S13 GX RX Interfacessyedsajjad68No ratings yet
- Mini Test PBD - SpeakingDocument4 pagesMini Test PBD - Speakinghe shaNo ratings yet
- Improving MV Underground Cable Performance - Experience of TNB MalaysiaDocument4 pagesImproving MV Underground Cable Performance - Experience of TNB Malaysialbk50No ratings yet
- Stone ColumnDocument116 pagesStone ColumnNur Farhana Ahmad Fuad100% (1)
- HUAWEI OCS Business Process Description PDFDocument228 pagesHUAWEI OCS Business Process Description PDFdidier_oNo ratings yet
- Method Statement For FDTDocument7 pagesMethod Statement For FDTMs UndergroundNo ratings yet
- Articles of Confederation LessonDocument2 pagesArticles of Confederation Lessonapi-233755289No ratings yet
- Calibration Procedure FOR Surface Plates Planekator Method: Technical ManualDocument11 pagesCalibration Procedure FOR Surface Plates Planekator Method: Technical Manualentico100% (1)
- GPS Equipment CalibrationDocument10 pagesGPS Equipment CalibrationAishah Drahman100% (1)
- 4D Asp: Wall Tiling 4D - PG 1Document3 pages4D Asp: Wall Tiling 4D - PG 1Vlaho AlamatNo ratings yet
- Add-On Effect of Brahmi in The Management of SchizophreniaDocument3 pagesAdd-On Effect of Brahmi in The Management of SchizophreniaNAITIKNo ratings yet
- Build A Cubic Meter LessonDocument3 pagesBuild A Cubic Meter Lessonapi-253637444No ratings yet
- Hostel Survey Analysis ReportDocument10 pagesHostel Survey Analysis ReportMoosa NaseerNo ratings yet
- Sequential StatementDocument12 pagesSequential Statementdineshvhaval100% (1)
- Author RefDocument12 pagesAuthor RefCihuy RahmatNo ratings yet