You might also like
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideFrom EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideNo ratings yet
- ThoracostomyDocument2 pagesThoracostomyJanelle MarceraNo ratings yet
- Registered Professional Nurse: Passbooks Study GuideFrom EverandRegistered Professional Nurse: Passbooks Study GuideNo ratings yet
- Chest Tube Thoracostomy ProcedureDocument17 pagesChest Tube Thoracostomy ProcedureJill Catherine CabanaNo ratings yet
- Chest DrainageDocument28 pagesChest DrainageCristy Guzman100% (1)
- Chest Tube Thoracostomy: Patient EducationDocument2 pagesChest Tube Thoracostomy: Patient EducationPhilippe Ceasar C. BascoNo ratings yet
- SuctioningDocument31 pagesSuctioningmelanie silvaNo ratings yet
- NURSING CARE OF ADULTS I: Passbooks Study GuideFrom EverandNURSING CARE OF ADULTS I: Passbooks Study GuideNo ratings yet
- Pharmacology Checklist - Rationale 02Document30 pagesPharmacology Checklist - Rationale 02Tisha DeiparineNo ratings yet
- 8 Irrigating A ColostomyDocument5 pages8 Irrigating A ColostomyAnn Jalover PerezNo ratings yet
- CYSTOCLYSISDocument1 pageCYSTOCLYSISzerpthederpNo ratings yet
- Nasogastric Tube Feeding GuideDocument74 pagesNasogastric Tube Feeding GuideGoddy Manzano100% (1)
- Assisting Adult Patient With Oral NutritionDocument2 pagesAssisting Adult Patient With Oral NutritionJoslyn GrossNo ratings yet
- What Is Crutch WalkingDocument3 pagesWhat Is Crutch WalkingMANANNo ratings yet
- NCM - CatheterizationDocument3 pagesNCM - CatheterizationYanna Habib-MangotaraNo ratings yet
- Emergency DrugsDocument47 pagesEmergency DrugsBesimanNo ratings yet
- Tracheostomy Care - An Evidence-Based Guide - American Nurse TodayDocument4 pagesTracheostomy Care - An Evidence-Based Guide - American Nurse TodayZulaikah Nur IstiqomahNo ratings yet
- Blood TransfusionDocument5 pagesBlood TransfusionNoel100% (4)
- Withdrawing Medication From An Ampule: EquipmentDocument6 pagesWithdrawing Medication From An Ampule: EquipmentMj Andayog100% (1)
- Caring for a Nephrostomy TubeDocument4 pagesCaring for a Nephrostomy TubeUmi KrisdyantiniNo ratings yet
- Removing A Nasogastric TubeDocument16 pagesRemoving A Nasogastric TubeBryJos tiongson100% (1)
- RBS and FBSDocument5 pagesRBS and FBSAllenne Rose Labja Vale100% (1)
- Nursing Pharmacology ReviewDocument8 pagesNursing Pharmacology ReviewKevin Mikhail EstandarteNo ratings yet
- EMERGENCY DRUGSDocument7 pagesEMERGENCY DRUGSJohn Balgoa100% (2)
- Changing An IV SolutionDocument2 pagesChanging An IV SolutionNoel100% (9)
- Drug Study On Emergency DrugsDocument14 pagesDrug Study On Emergency Drugsjcarysuitos100% (4)
- Understanding IV FluidsDocument2 pagesUnderstanding IV FluidsJoe Anne Maniulit, MSN, RN100% (5)
- Tracheostomy Suctioning SkillDocument6 pagesTracheostomy Suctioning Skill3thanKimNo ratings yet
- Copd Case StudyDocument6 pagesCopd Case StudyDivine ParagasNo ratings yet
- Responsibilites of A PACU NurseDocument1 pageResponsibilites of A PACU NurseTarquin TomadaNo ratings yet
- CNA - Code of Ethics 2008Document64 pagesCNA - Code of Ethics 2008Andreas AndrellisNo ratings yet
- Group 5 - Hemodialysis - Chronic Kidney FailureDocument31 pagesGroup 5 - Hemodialysis - Chronic Kidney FailureKimberly Abella CabreraNo ratings yet
- Flucloxacillin AFTcapssolnDocument6 pagesFlucloxacillin AFTcapssolnEliza ArmanNo ratings yet
- ) Administering Nasogastric Tube or Orogastric Tube FeedingDocument6 pages) Administering Nasogastric Tube or Orogastric Tube FeedingJohn Pearl FernandezNo ratings yet
- Pharamacology Notes 3Document7 pagesPharamacology Notes 3Martinet CalvertNo ratings yet
- Care For Patient With ColostomyDocument4 pagesCare For Patient With ColostomyJoseph C. CanielNo ratings yet
- Measuring Central Venous PressureDocument10 pagesMeasuring Central Venous PressureRaghu RajanNo ratings yet
- Chest Tubes: Indications, Placement and CareDocument76 pagesChest Tubes: Indications, Placement and CareMarites Santos AquinoNo ratings yet
- Nasogastric Tube (NGT) InsertionDocument19 pagesNasogastric Tube (NGT) InsertionNorman VerdeflorNo ratings yet
- Administering EnemaDocument35 pagesAdministering Enemabajaoc100% (1)
- IV TherapyDocument15 pagesIV TherapyJojebelle Kate Iyog-cabanlet100% (1)
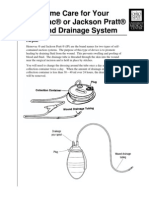
- Jackson PrattDocument7 pagesJackson PrattjulialeoNo ratings yet
- OxygenationDocument20 pagesOxygenationKhie-An OcampoNo ratings yet
- Description: Congestive Heart FailureDocument22 pagesDescription: Congestive Heart FailurePinklet Arleena CubianNo ratings yet
- Cardiac MonitoringDocument19 pagesCardiac MonitoringYaska Musa100% (1)
- Fecal ImpactionDocument5 pagesFecal Impactioncharie2No ratings yet
- IV ComputationDocument12 pagesIV Computationapi-300218860100% (1)
- Administration of Inotropes Evidence Based Nursing PolicyDocument8 pagesAdministration of Inotropes Evidence Based Nursing PolicyRonald ThakorNo ratings yet
- Nebu&CPTDocument32 pagesNebu&CPTAbigail Bantayan100% (1)
- Insulin AdministrationDocument15 pagesInsulin Administrationmec17No ratings yet
- Evolution of Nursing Research and Role of The Nurse in ResearchDocument3 pagesEvolution of Nursing Research and Role of The Nurse in ResearchAlmer OstreaNo ratings yet
- Chest Tube Insertion and MonitoringDocument4 pagesChest Tube Insertion and MonitoringCamille Cirineo Arensol100% (2)
- Chest Tube Drainage Systems ExplainedDocument3 pagesChest Tube Drainage Systems Explainedparislove19No ratings yet
- Tube ThoracostomyDocument17 pagesTube ThoracostomyheiyuNo ratings yet
- Chest Tube DrainageDocument45 pagesChest Tube DrainageDonald BidenNo ratings yet
- Management of Chest TubeDocument22 pagesManagement of Chest TubeFatima Hafza SahiddinNo ratings yet
- Chest Tube and Water-Seal DrainageDocument25 pagesChest Tube and Water-Seal DrainageGhadaNo ratings yet
- Skills LabDocument107 pagesSkills LabskybluealiNo ratings yet
- Skills Lab Presentation 4Document32 pagesSkills Lab Presentation 4skybluealiNo ratings yet
- Pulse OximeterDocument3 pagesPulse OximeterskybluealiNo ratings yet
- Insulin AdministrationDocument8 pagesInsulin AdministrationskybluealiNo ratings yet
- Arterial Blood Gas ReportDocument8 pagesArterial Blood Gas ReportskybluealiNo ratings yet
- Final Exam Questions 3Document40 pagesFinal Exam Questions 3clarke skaikruNo ratings yet
- Atls® Written Pretest 10th Edition: 684 Section 4 Student Course ResourcesDocument9 pagesAtls® Written Pretest 10th Edition: 684 Section 4 Student Course ResourcesIB leaksNo ratings yet
- Respiratory Examination OSCE GuideDocument14 pagesRespiratory Examination OSCE GuideSam James100% (1)
- Human Diseases Case Study 19CDocument3 pagesHuman Diseases Case Study 19Cairickann50% (2)
- Lung conditions: Atelectasis, tuberculosis, abscess and pleural effusionDocument14 pagesLung conditions: Atelectasis, tuberculosis, abscess and pleural effusionSasha IfahmyNo ratings yet
- 3B Scientific Medical Education 2018 enDocument276 pages3B Scientific Medical Education 2018 enHari YantoNo ratings yet
- New MCQDocument129 pagesNew MCQAlhajiNo ratings yet
- CH 46 Complications of AnaesthesiaDocument29 pagesCH 46 Complications of AnaesthesiaChristian LeepoNo ratings yet
- Clinical Management of TB and HIVDocument154 pagesClinical Management of TB and HIVapi-3781623100% (3)
- Principles in Trauma ManagementDocument34 pagesPrinciples in Trauma Managementvirz23No ratings yet
- Kuliah Radiologi Cardiorespiratory 2Document99 pagesKuliah Radiologi Cardiorespiratory 2Muhammad Sandy Ali YafieNo ratings yet
- UHS-OSPE of Medicine (Annual 2009Document13 pagesUHS-OSPE of Medicine (Annual 2009Latif RanaNo ratings yet
- TCCC Quick Reference Guide 2017Document54 pagesTCCC Quick Reference Guide 2017tzimistigris100% (1)
- Resp Lecture NotesDocument18 pagesResp Lecture Notessurviving nursing schoolNo ratings yet
- General Practitioner - Pulmonology MCQsDocument37 pagesGeneral Practitioner - Pulmonology MCQsAsif Newaz100% (7)
- filePV 31 05 232Document11 pagesfilePV 31 05 232Raul Hernandez SotoNo ratings yet
- Medical Surgical Nursing Assignment - 2Document147 pagesMedical Surgical Nursing Assignment - 2Sonali Sengar0% (1)
- The Impact of Cannabis On Your Lungs - BLF Report 2012 PDFDocument19 pagesThe Impact of Cannabis On Your Lungs - BLF Report 2012 PDFtomaz_filhoNo ratings yet
- Accepted Manuscript: 10.1016/j.cpem.2018.02.009Document41 pagesAccepted Manuscript: 10.1016/j.cpem.2018.02.009Richo WijayaNo ratings yet
- Examination of Respiratory SystemDocument78 pagesExamination of Respiratory Systemwidya sri hastutiNo ratings yet
- Evaluation and initial approach to undifferentiated hypotension and shockDocument34 pagesEvaluation and initial approach to undifferentiated hypotension and shockمحمد زينNo ratings yet
- System Disorder: PneumothoraxDocument1 pageSystem Disorder: PneumothoraxEli ReyesNo ratings yet
- Post Tubercular Sequelae.123175034Document29 pagesPost Tubercular Sequelae.123175034Andre Prasetyo MahesyaNo ratings yet
- IS0871 - Combat Lifesaver Course - Student Self-StudyDocument200 pagesIS0871 - Combat Lifesaver Course - Student Self-StudyChad Vander VenNo ratings yet
- Pneumothorax & TBI Care After MVADocument36 pagesPneumothorax & TBI Care After MVAdustin_camposNo ratings yet
- MCI Drill Sample ScenariosDocument8 pagesMCI Drill Sample ScenariosDarylNo ratings yet
- A&e Test - ATLSDocument14 pagesA&e Test - ATLSAnonymous x0P332K5uu86% (14)
- RS McqsDocument6 pagesRS McqsMuhammad Farrukh ul IslamNo ratings yet
- Zanki Respiratory PathologyDocument15 pagesZanki Respiratory Pathologysmian08100% (1)
- Giant Pulmonary Bullae in Children: Journal of Pediatric Surgery Case Reports July 2020Document7 pagesGiant Pulmonary Bullae in Children: Journal of Pediatric Surgery Case Reports July 2020SOPHIASTIA KUSBIANTI MHS 2017No ratings yet
- Functional Safety from Scratch: A Practical Guide to Process Industry ApplicationsFrom EverandFunctional Safety from Scratch: A Practical Guide to Process Industry ApplicationsNo ratings yet
- Guidelines for Implementing Process Safety ManagementFrom EverandGuidelines for Implementing Process Safety ManagementNo ratings yet
- Guidelines for Initiating Events and Independent Protection Layers in Layer of Protection AnalysisFrom EverandGuidelines for Initiating Events and Independent Protection Layers in Layer of Protection AnalysisRating: 5 out of 5 stars5/5 (1)
- Practical Industrial Safety, Risk Assessment and Shutdown SystemsFrom EverandPractical Industrial Safety, Risk Assessment and Shutdown SystemsRating: 4 out of 5 stars4/5 (11)
- Nutritional and Therapeutic Interventions for Diabetes and Metabolic SyndromeFrom EverandNutritional and Therapeutic Interventions for Diabetes and Metabolic SyndromeNo ratings yet
- A Complete Guide to Safety Officer Interview Questions and AnswersFrom EverandA Complete Guide to Safety Officer Interview Questions and AnswersRating: 4 out of 5 stars4/5 (1)
- Guidelines for Auditing Process Safety Management SystemsFrom EverandGuidelines for Auditing Process Safety Management SystemsNo ratings yet
- A Poison Like No Other: How Microplastics Corrupted Our Planet and Our BodiesFrom EverandA Poison Like No Other: How Microplastics Corrupted Our Planet and Our BodiesRating: 5 out of 5 stars5/5 (1)
- Introduction to Petroleum Process SafetyFrom EverandIntroduction to Petroleum Process SafetyRating: 3 out of 5 stars3/5 (2)
- Trevor Kletz Compendium: His Process Safety Wisdom Updated for a New GenerationFrom EverandTrevor Kletz Compendium: His Process Safety Wisdom Updated for a New GenerationNo ratings yet
- Inherently Safer Chemical Processes: A Life Cycle ApproachFrom EverandInherently Safer Chemical Processes: A Life Cycle ApproachRating: 5 out of 5 stars5/5 (1)
- Rules of Thumb for Maintenance and Reliability EngineersFrom EverandRules of Thumb for Maintenance and Reliability EngineersRating: 4.5 out of 5 stars4.5/5 (12)
- Incidents That Define Process SafetyFrom EverandIncidents That Define Process SafetyNo ratings yet
- Safety Fundamentals and Best Practices in Construction IndustryFrom EverandSafety Fundamentals and Best Practices in Construction IndustryNo ratings yet
- Radium Girls: Women and Industrial Health Reform, 1910-1935From EverandRadium Girls: Women and Industrial Health Reform, 1910-1935Rating: 4.5 out of 5 stars4.5/5 (4)
- Chemical Process Safety: Learning from Case HistoriesFrom EverandChemical Process Safety: Learning from Case HistoriesRating: 4 out of 5 stars4/5 (14)
- The ISO 45001:2018 Implementation Handbook: Guidance on Building an Occupational Health and Safety Management SystemFrom EverandThe ISO 45001:2018 Implementation Handbook: Guidance on Building an Occupational Health and Safety Management SystemNo ratings yet
- Exercise, Sport, and Bioanalytical Chemistry: Principles and PracticeFrom EverandExercise, Sport, and Bioanalytical Chemistry: Principles and PracticeNo ratings yet
- 3D Printing of Concrete: State of the Art and Challenges of the Digital Construction RevolutionFrom Everand3D Printing of Concrete: State of the Art and Challenges of the Digital Construction RevolutionArnaud PerrotNo ratings yet
- One Health: Integrated Approach to 21st Century Challenges to HealthFrom EverandOne Health: Integrated Approach to 21st Century Challenges to HealthJoana C. PrataNo ratings yet
- Autophagy in Health and DiseaseFrom EverandAutophagy in Health and DiseaseBeverly RothermelNo ratings yet
- The Safety Critical Systems Handbook: A Straightforward Guide to Functional Safety: IEC 61508 (2010 Edition), IEC 61511 (2015 Edition) and Related GuidanceFrom EverandThe Safety Critical Systems Handbook: A Straightforward Guide to Functional Safety: IEC 61508 (2010 Edition), IEC 61511 (2015 Edition) and Related GuidanceRating: 5 out of 5 stars5/5 (1)
- Safety and Intelligent Transport Systems Development in the People’s Republic of ChinaFrom EverandSafety and Intelligent Transport Systems Development in the People’s Republic of ChinaNo ratings yet