You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Infants and ToddlersDocument14 pagesInfants and ToddlersJosias Smith100% (1)
- Stroke RecoveryDocument20 pagesStroke RecoveryVanessa SnowNo ratings yet
- Honey Nut Baklava Filo Pastry TreatsDocument2 pagesHoney Nut Baklava Filo Pastry TreatsiantperNo ratings yet
- Burns SeminarDocument66 pagesBurns SeminarPratibha Thakur100% (1)
- Day 4 Nurses NotesDocument11 pagesDay 4 Nurses Notesapi-265625311No ratings yet
- Day 3 Nurses NotesDocument11 pagesDay 3 Nurses Notesapi-265625311No ratings yet
- Day 1 Nurses NotesDocument13 pagesDay 1 Nurses Notesapi-265625311100% (1)
- Ccc-Inpatient Hospital Day 4-Med SurgDocument1 pageCcc-Inpatient Hospital Day 4-Med Surgapi-265625311No ratings yet
- Ccc-Inpatient Hospital Day 4-Med SurgDocument1 pageCcc-Inpatient Hospital Day 4-Med Surgapi-265625311No ratings yet
- CCC - Inpatient Hospital Day 3 - IcuDocument2 pagesCCC - Inpatient Hospital Day 3 - Icuapi-265625311No ratings yet
- CCC - Inpatient Hospital Day 3 - IcuDocument2 pagesCCC - Inpatient Hospital Day 3 - Icuapi-265625311No ratings yet
- Ccc-Inpatient Hospital Day 1-Med SurgDocument2 pagesCcc-Inpatient Hospital Day 1-Med Surgapi-265625311No ratings yet
- Labs - Sherman RoderDocument2 pagesLabs - Sherman Roderapi-265625311No ratings yet
- Homes & Diamonds of Liz TaylorDocument42 pagesHomes & Diamonds of Liz TaylorFridayFunStuffNo ratings yet
- Experimental Animals Vol1Document209 pagesExperimental Animals Vol1JohnNo ratings yet
- GSR (ROAD) 2015Document74 pagesGSR (ROAD) 2015Gautam RaiNo ratings yet
- CEU - Catalytic ReactorsDocument3 pagesCEU - Catalytic ReactorsPong VongNo ratings yet
- LAOKEN Comparison With J&JDocument3 pagesLAOKEN Comparison With J&JMario Alfonso MartinezNo ratings yet
- Sohail KhanDocument3 pagesSohail KhanRashid Muhammad SarwarNo ratings yet
- NTTM632 Anand Informatica-ETL Lead ResumeDocument8 pagesNTTM632 Anand Informatica-ETL Lead ResumeMohammed JawadNo ratings yet
- Vitamin D DeficinyDocument11 pagesVitamin D DeficinyسالمNo ratings yet
- Oral Dislocation Rehabilitation Program - FirstDocument2 pagesOral Dislocation Rehabilitation Program - FirstPriyaki SebastianNo ratings yet
- An Interview - ExercisesDocument3 pagesAn Interview - ExercisesCarmen GloriaNo ratings yet
- Plant Nematology: A Briefly IntroductionDocument463 pagesPlant Nematology: A Briefly IntroductionRodrigo CarralNo ratings yet
- Shavuot 5774Document4 pagesShavuot 5774Andrea KingNo ratings yet
- The Evolution of FungiDocument15 pagesThe Evolution of Fungi2010eon2010No ratings yet
- Saloni Shah - LLM DissertationDocument156 pagesSaloni Shah - LLM DissertationNilesh BatraNo ratings yet
- Schedule Examination 2010 2011Document5 pagesSchedule Examination 2010 2011pawan15588rediffmailNo ratings yet
- TDDDocument4 pagesTDDJay VibhaniNo ratings yet
- Quality and Functionality of Excipients-Art (Alumnos-S) PDFDocument14 pagesQuality and Functionality of Excipients-Art (Alumnos-S) PDFLaura PerezNo ratings yet
- Multiple Bank Accounts Registration FormDocument2 pagesMultiple Bank Accounts Registration FormAjith JainNo ratings yet
- MAstering IATFDocument20 pagesMAstering IATFGyanesh_DBNo ratings yet
- 22Document22 pages22vanhau24No ratings yet
- Dermato Venerology ScienceDocument11 pagesDermato Venerology ScienceAQis AQishNo ratings yet
- LENZE E84AVxCx - 8400 StateLine-HighLine-TopLine 0.25-45kW - v9-0 - ENDocument291 pagesLENZE E84AVxCx - 8400 StateLine-HighLine-TopLine 0.25-45kW - v9-0 - ENClaudioNo ratings yet
- Deped Memo No. 165, S 2010: WastedDocument6 pagesDeped Memo No. 165, S 2010: WastedJayne InoferioNo ratings yet
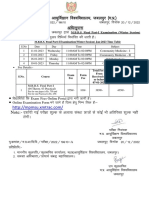
- MBBS Final Part-I (Winter Session) Time Table (Jan 2023)Document1 pageMBBS Final Part-I (Winter Session) Time Table (Jan 2023)crystal mindNo ratings yet
- Entrenamiento de Fuerza y Salud Pediátrica Ingles PDFDocument9 pagesEntrenamiento de Fuerza y Salud Pediátrica Ingles PDFGiiovanny PardoNo ratings yet
- Evonik-BREAK THRU Brochure Microbials EN Asset 2214205Document5 pagesEvonik-BREAK THRU Brochure Microbials EN Asset 2214205李雷No ratings yet