You might also like
- Trial Registration Form Season 2017: Girls & Senior Womens SoccerDocument2 pagesTrial Registration Form Season 2017: Girls & Senior Womens SoccerBiancaNo ratings yet
- Trial Athlete - Ndlac: Welcome To Northern Districts Little Athletics CentreDocument1 pageTrial Athlete - Ndlac: Welcome To Northern Districts Little Athletics CentreAnonymous Re62LKaACNo ratings yet
- 2016 Fall Rec RegistrationDocument2 pages2016 Fall Rec Registrationapi-243976788No ratings yet
- 2024 Senior Registration FormDocument2 pages2024 Senior Registration Formoliver123456321No ratings yet
- 2024 Senior Registration FormDocument2 pages2024 Senior Registration Formoliver123456321No ratings yet
- South Australian Church Basketball Association Inc.: Email Address: (Please Print Clearly)Document6 pagesSouth Australian Church Basketball Association Inc.: Email Address: (Please Print Clearly)Eric MontgomeryNo ratings yet
- NBO 2016 RegistrationDocument2 pagesNBO 2016 RegistrationMelissa McGregorNo ratings yet
- Ryba 2012 Signup FormDocument1 pageRyba 2012 Signup FormGil SmartNo ratings yet
- Alumni Game Participant RegistrationDocument1 pageAlumni Game Participant RegistrationMelanie HayesNo ratings yet
- Nomination Form For Boys Cricket Trials 2011Document2 pagesNomination Form For Boys Cricket Trials 2011Sandwell Cricket LeagueNo ratings yet
- RFU Young Player Registration FormDocument1 pageRFU Young Player Registration FormMalcolm WilsonNo ratings yet
- Cedar Valley Soccer Association Order 685120 ReceiptDocument2 pagesCedar Valley Soccer Association Order 685120 ReceiptKyle Allen SchulzNo ratings yet
- Nomination FormsDocument7 pagesNomination Formsapi-300607857No ratings yet
- FOD Membership ApplicationDocument1 pageFOD Membership ApplicationBill DozierNo ratings yet
- Work Experience Application Form 2018Document3 pagesWork Experience Application Form 2018SofiaNo ratings yet
- PTH Registration SummerDocument2 pagesPTH Registration SummerBarbara MacLeod Junior Club CaptainNo ratings yet
- HADARC Mem FormDocument1 pageHADARC Mem FormpatriotactorNo ratings yet
- Data Protection New Law 2018 1Document1 pageData Protection New Law 2018 1Brian HumphriesNo ratings yet
- 2011 Basketball RegistrationDocument3 pages2011 Basketball RegistrationBelvidere GreenNo ratings yet
- MCC Membership APP Form 2Document2 pagesMCC Membership APP Form 23187265No ratings yet
- TennisfillableformDocument2 pagesTennisfillableformapi-288575650No ratings yet
- Application Form KYSBDocument2 pagesApplication Form KYSBHaziq ShafNo ratings yet
- Provincial Orders Form 2023Document2 pagesProvincial Orders Form 2023mkenhle5No ratings yet
- Hoyahof Nomination Form 2017-18Document3 pagesHoyahof Nomination Form 2017-18api-377837206No ratings yet
- UWA Tennis Club Membership FormDocument3 pagesUWA Tennis Club Membership FormTony CunninghamNo ratings yet
- 2010 Aflq Player Rego FormDocument2 pages2010 Aflq Player Rego FormJenna VandykNo ratings yet
- SponsorshipDocument1 pageSponsorshipapi-240233692No ratings yet
- Usa Swimming 2020 Non-Athlete Registration Application LSC: AlaskaDocument1 pageUsa Swimming 2020 Non-Athlete Registration Application LSC: AlaskaJohnNo ratings yet
- Penticton Athletics Track and Field Club Registration Form UpdatedDocument1 pagePenticton Athletics Track and Field Club Registration Form Updatedapi-256034770No ratings yet
- BCBS Fitness Benefit Form PDFDocument2 pagesBCBS Fitness Benefit Form PDFlalabaiNo ratings yet
- Welcome To Season 2015 - 2016: Upcoming EventsDocument6 pagesWelcome To Season 2015 - 2016: Upcoming EventsGreg O'MearaNo ratings yet
- PRC Membership Application-CDocument1 pagePRC Membership Application-CwoodlandsuperNo ratings yet
- Youth Basketball League Registration FormDocument2 pagesYouth Basketball League Registration FormAimee Lyness CornettNo ratings yet
- ApplicationsfuDocument5 pagesApplicationsfuapi-372310429No ratings yet
- RWTW RunDocument5 pagesRWTW Runapi-262803234No ratings yet
- Junior Membership Form NewDocument3 pagesJunior Membership Form NewStacey CliffordNo ratings yet
- Excel Gantt Chart TemplateDocument4 pagesExcel Gantt Chart Templatejunaid_jdNo ratings yet
- Upward Brochure 2011-2012Document1 pageUpward Brochure 2011-2012Stillwater's Community ConnectionNo ratings yet
- Vasa Membership Application Usa 2013Document1 pageVasa Membership Application Usa 2013api-287229788No ratings yet
- 3 3 For Chinatown: When: Where: SponsorDocument2 pages3 3 For Chinatown: When: Where: SponsoreeddwinNo ratings yet
- Little League Info 2016Document2 pagesLittle League Info 2016RESprincipalNo ratings yet
- Individual DTPC Registration FormDocument2 pagesIndividual DTPC Registration FormrichfosterralieNo ratings yet
- Sussex Central Wrestling Pee-Wee/Youth Clinic July 9-13, 2012Document2 pagesSussex Central Wrestling Pee-Wee/Youth Clinic July 9-13, 2012api-121967263No ratings yet
- Awana Registration Medical Release Form 2011Document1 pageAwana Registration Medical Release Form 2011api-47607773No ratings yet
- RegistrationDocument1 pageRegistrationapi-212480101No ratings yet
- Recruit Questionnaire SoccerDocument2 pagesRecruit Questionnaire SoccerVisnuMaharajNo ratings yet
- Fact SheetDocument3 pagesFact Sheetapi-258030892No ratings yet
- 2011 Combine Player FormDocument1 page2011 Combine Player Formobama mammaNo ratings yet
- Application Form Mini X-Plorace Kca'11Document3 pagesApplication Form Mini X-Plorace Kca'11Jat KimieNo ratings yet
- Team Registration Information: October 21-23, 2011 The 949 Roller Hockey Center - Irvine, CADocument4 pagesTeam Registration Information: October 21-23, 2011 The 949 Roller Hockey Center - Irvine, CAbcohenjrNo ratings yet
- Liverpool Supporters Club Malaysia Membership FormDocument1 pageLiverpool Supporters Club Malaysia Membership FormAsran SaripNo ratings yet
- Hs Club EligDocument1 pageHs Club Eligapi-263192676No ratings yet
- PDF Soccer Registration Forms 2015 PDFDocument3 pagesPDF Soccer Registration Forms 2015 PDFChrisNo ratings yet
- Application Form 2011 SeasonDocument2 pagesApplication Form 2011 SeasonTooba AamirNo ratings yet
- Double The Pride FinalDocument2 pagesDouble The Pride FinallearnmpNo ratings yet
- ASA South West Bursary Scheme 2011-2012: Application Pack - Step by Step GuideDocument5 pagesASA South West Bursary Scheme 2011-2012: Application Pack - Step by Step GuidesportsnetworkNo ratings yet
- Join Phelps Chess ClubDocument3 pagesJoin Phelps Chess Club3187265No ratings yet
- FCSD DonationwebsiteformDocument1 pageFCSD Donationwebsiteformapi-463973679No ratings yet
- Nhem Paul Sokum 1981 CambodiaDocument24 pagesNhem Paul Sokum 1981 Cambodiathe missions networkNo ratings yet
- Maps 4 Up - Merged With Directions2016Document3 pagesMaps 4 Up - Merged With Directions2016norriekrNo ratings yet
- Maps 4 Up - Merged With Directions 2016Document3 pagesMaps 4 Up - Merged With Directions 2016norriekrNo ratings yet
- Maps 4 Up - Merged With Directions 2015Document3 pagesMaps 4 Up - Merged With Directions 2015norriekrNo ratings yet
- LAC - xc.2015 Flyer For WebDocument2 pagesLAC - xc.2015 Flyer For WebnorriekrNo ratings yet
- LAC - xc.2014 Flyer For WebDocument2 pagesLAC - xc.2014 Flyer For WebnorriekrNo ratings yet
- Membership Renewal Form With ConsentDocument2 pagesMembership Renewal Form With ConsentnorriekrNo ratings yet
- Membership Renewal Consent FormDocument2 pagesMembership Renewal Consent FormnorriekrNo ratings yet
- LAC - xc.2016 Flyer For WebDocument2 pagesLAC - xc.2016 Flyer For WebnorriekrNo ratings yet
- Maps 4 Up - Merged With Directions 2015Document3 pagesMaps 4 Up - Merged With Directions 2015norriekrNo ratings yet
- Membership Renewal Form With ConsentDocument2 pagesMembership Renewal Form With ConsentnorriekrNo ratings yet
- Newsletter April 2014Document4 pagesNewsletter April 2014norriekrNo ratings yet
- Lac 10 Mile RR 2014 Results Inc TeamsDocument6 pagesLac 10 Mile RR 2014 Results Inc TeamsnorriekrNo ratings yet
- Membership Renewal Form With ConsentDocument2 pagesMembership Renewal Form With ConsentnorriekrNo ratings yet
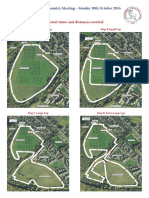
- Laps, Courses and Directions To The VenueDocument3 pagesLaps, Courses and Directions To The VenuenorriekrNo ratings yet
- Membership Renewal FormDocument1 pageMembership Renewal FormnorriekrNo ratings yet
- Danny Burnett IntroDocument1 pageDanny Burnett IntronorriekrNo ratings yet
- LAC - xc.2013 Flyer For Web - Merged With DirectionsDocument3 pagesLAC - xc.2013 Flyer For Web - Merged With DirectionsnorriekrNo ratings yet
- LAC Road Race 2014 FlyerDocument4 pagesLAC Road Race 2014 FlyernorriekrNo ratings yet
- Under 11 Girls: Place Race No. Name Club TimeDocument9 pagesUnder 11 Girls: Place Race No. Name Club TimenorriekrNo ratings yet
- Lac X Country Result Sun Scrutinised 2012Document9 pagesLac X Country Result Sun Scrutinised 2012norriekrNo ratings yet
- Competitive Opportunities 2013Document14 pagesCompetitive Opportunities 2013norriekrNo ratings yet
- AGM LetterDocument1 pageAGM LetternorriekrNo ratings yet
- LAC - XC.2012 A5 FlyerDocument2 pagesLAC - XC.2012 A5 FlyernorriekrNo ratings yet
- Lac X Country Result Sun Scrutinised 2012Document9 pagesLac X Country Result Sun Scrutinised 2012norriekrNo ratings yet
- Gore-Glen, Gorebridge Lasswade AC 30th Open Cross Country Event 6th November, 2011Document8 pagesGore-Glen, Gorebridge Lasswade AC 30th Open Cross Country Event 6th November, 2011norriekrNo ratings yet
- Athletics Needs YouDocument1 pageAthletics Needs YounorriekrNo ratings yet
- Lasswade Athletics Club 10 Mile Road Race 2012: Place Race No. Name Club Time Cat MidlothianDocument7 pagesLasswade Athletics Club 10 Mile Road Race 2012: Place Race No. Name Club Time Cat MidlothiannorriekrNo ratings yet
- Lasswade Athletics Club 10 Mile Road Race 2012: Place Race No. Name Club Time Cat MidlothianDocument7 pagesLasswade Athletics Club 10 Mile Road Race 2012: Place Race No. Name Club Time Cat MidlothiannorriekrNo ratings yet
- LAC XC 2011 A5 Flyer New - MergedDocument5 pagesLAC XC 2011 A5 Flyer New - MergednorriekrNo ratings yet