You might also like
- Ebstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandEbstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Cardiovascular System: By: S@JDocument35 pagesCardiovascular System: By: S@JD TekNo ratings yet
- Abnormal Slow Heart Beats, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandAbnormal Slow Heart Beats, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Cardiovascular Definitions and Exam TechniquesDocument7 pagesCardiovascular Definitions and Exam TechniquesDestinee CapleNo ratings yet
- LEC 15.1 - Abdominal HerniasDocument37 pagesLEC 15.1 - Abdominal HerniasTudor CorneaNo ratings yet
- Aquifer InternalMedicine09 - 55Document7 pagesAquifer InternalMedicine09 - 55JulieNo ratings yet
- A Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsNo ratings yet
- IM 3A PE Cardiology Dr. JumangitDocument12 pagesIM 3A PE Cardiology Dr. JumangitCzara DyNo ratings yet
- Clinical Examination of The AbdomenDocument13 pagesClinical Examination of The AbdomenNur Miladiyah100% (1)
- Examination of A StomaDocument3 pagesExamination of A StomaChloe100% (1)
- Intra Abdominal 2009Document8 pagesIntra Abdominal 2009Shinta Dwi Septiani Putri WibowoNo ratings yet
- Cardio AssessmentDocument2 pagesCardio AssessmentMabesNo ratings yet
- Aquifer InternalMedicine11 - 45Document8 pagesAquifer InternalMedicine11 - 45JulieNo ratings yet
- Pre-And Post-Book Study Test For The Shelf Exam: How To Use This ChapterDocument6 pagesPre-And Post-Book Study Test For The Shelf Exam: How To Use This ChapterMiguel CuevasNo ratings yet
- Reye's SyndromeDocument11 pagesReye's SyndromeChristine Go100% (1)
- Systemic Surgery NuggetsDocument17 pagesSystemic Surgery NuggetsAhmad UsmanNo ratings yet
- Family Medicine 33: 28-Year-Old Female With Dizziness: Learning ObjectivesDocument6 pagesFamily Medicine 33: 28-Year-Old Female With Dizziness: Learning ObjectivesAndrea Kristin OrigenesNo ratings yet
- Local Chest Examination AMM2Document37 pagesLocal Chest Examination AMM2saeedoofNo ratings yet
- HyphemaDocument19 pagesHyphemaLiyanti RinceNo ratings yet
- Stoma Examination OSCE GuideDocument5 pagesStoma Examination OSCE GuideEssa AfridiNo ratings yet
- PericarditisDocument29 pagesPericarditisPavin KumarNo ratings yet
- Drug Toxicity and PoisoningDocument12 pagesDrug Toxicity and PoisoningPAULA MARIE MERCADO LLIDONo ratings yet
- Pulmo ThromboembolismDocument34 pagesPulmo ThromboembolismAlexander Santiago ParelNo ratings yet
- Acute AbdomenDocument19 pagesAcute AbdomenNazmi Z. MehmetiNo ratings yet
- Approach To Ventricular ArrhythmiasDocument18 pagesApproach To Ventricular ArrhythmiasDavid CruzNo ratings yet
- Thyroid Exam OSCEDocument4 pagesThyroid Exam OSCEJon Mark LimNo ratings yet
- History Taking and Physical Examination of Cardiovascular System-The EssentialsDocument72 pagesHistory Taking and Physical Examination of Cardiovascular System-The EssentialsReena Joanella TimbreNo ratings yet
- Cardiovascular BigDocument37 pagesCardiovascular Bigfaiz nasirNo ratings yet
- Long Case PDFDocument8 pagesLong Case PDFAbdulrahman Mohamed GhanimNo ratings yet
- X Thorax BeoordelenDocument135 pagesX Thorax BeoordelenmtescasuraNo ratings yet
- Recurrent UTI Case Presentation in Child with Obstructive UropathyDocument26 pagesRecurrent UTI Case Presentation in Child with Obstructive UropathyAminath MeesanNo ratings yet
- Abnormal Pulse FindingsDocument43 pagesAbnormal Pulse FindingsAngelo LacisteNo ratings yet
- Cardiac Exam Guide: Inspection, Palpation, AuscultationDocument23 pagesCardiac Exam Guide: Inspection, Palpation, AuscultationAreza Eka PermanaNo ratings yet
- Atelectasis: Contraction Atelectasis (Or Cicatrization Atelectasis)Document10 pagesAtelectasis: Contraction Atelectasis (Or Cicatrization Atelectasis)Gan BangNo ratings yet
- History and Physical Examination TemplateDocument3 pagesHistory and Physical Examination TemplateRawa MuhsinNo ratings yet
- Place a chest tubeDocument83 pagesPlace a chest tubehwelpNo ratings yet
- Lung AuscultationDocument62 pagesLung AuscultationOlea CroitorNo ratings yet
- History and Examinatoin of The Cardiovascular SystemDocument47 pagesHistory and Examinatoin of The Cardiovascular Systemmawada abdallaNo ratings yet
- Cardiovascular System Diseases Part 1Document22 pagesCardiovascular System Diseases Part 1Prince Rener Velasco PeraNo ratings yet
- Chest Trauma FinalDocument50 pagesChest Trauma FinalAsim Siddiq VineNo ratings yet
- Shivaani (Internal Medicine CWU)Document12 pagesShivaani (Internal Medicine CWU)S.M. Manogaran Shivaani AP S.M. ManogaranNo ratings yet
- History Taking Cheat SheetDocument1 pageHistory Taking Cheat SheetLaura ForsythNo ratings yet
- CVS II Tutorials Apr 12-17Document7 pagesCVS II Tutorials Apr 12-17rishitNo ratings yet
- Chest Pain: Sumit Bose, MD PGY-3Document55 pagesChest Pain: Sumit Bose, MD PGY-3Irfan100% (1)
- Diseases of the Aorta: Causes and Types of Aortic AneurysmsDocument11 pagesDiseases of the Aorta: Causes and Types of Aortic AneurysmsMedisina101No ratings yet
- Differential Diagnosis of Valvular Heart DiseaseDocument10 pagesDifferential Diagnosis of Valvular Heart DiseaseAbhisek ChatterjeeNo ratings yet
- Gyne Case COCDocument37 pagesGyne Case COCLian BaylosisNo ratings yet
- GP Reg - Asthma and Spirometry 2011Document114 pagesGP Reg - Asthma and Spirometry 2011minerva_stanciuNo ratings yet
- Heart MurmursDocument48 pagesHeart MurmursAhmed T Al-MomtinNo ratings yet
- Cardiology A. Woo PDFDocument52 pagesCardiology A. Woo PDFiuliNo ratings yet
- Cardiac Pathophysiology: Understanding Heart ConditionsDocument83 pagesCardiac Pathophysiology: Understanding Heart ConditionsJauhar Anindita SariNo ratings yet
- Congenital Heart DiseaseDocument10 pagesCongenital Heart DiseaseMarisa PetersonNo ratings yet
- Sudden Maternal Collapse: Max Brinsmead MB Bs PHD May 2015Document23 pagesSudden Maternal Collapse: Max Brinsmead MB Bs PHD May 2015DrChauhanNo ratings yet
- Posterior Cranial Fossa Anesthetic ManagementDocument48 pagesPosterior Cranial Fossa Anesthetic ManagementDivya Rekha KolliNo ratings yet
- Aorta DissectionDocument98 pagesAorta DissectionDian SukaryaNo ratings yet
- أدوية الطوارىءDocument162 pagesأدوية الطوارىءManar22No ratings yet
- Shock, Sirs & ModsDocument37 pagesShock, Sirs & ModsambitioustamannaNo ratings yet
- Bloom SyndromeDocument2 pagesBloom SyndromeDrMubashir ShaikhNo ratings yet
- Heart FailureDocument7 pagesHeart FailurestudymedicNo ratings yet
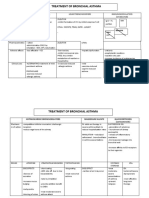
- Treatment of Bronchial AsthmaDocument3 pagesTreatment of Bronchial AsthmastudymedicNo ratings yet
- First Line Agents (Essentials) in Treatment of TBDocument2 pagesFirst Line Agents (Essentials) in Treatment of TBstudymedicNo ratings yet
- History Taking in Pulmonary MedicineDocument14 pagesHistory Taking in Pulmonary MedicinestudymedicNo ratings yet
- Introduction To Platyhelminthes (Flukes)Document78 pagesIntroduction To Platyhelminthes (Flukes)studymedicNo ratings yet
- Jugular VeinsDocument13 pagesJugular VeinsstudymedicNo ratings yet
- Symptoms of CvsDocument25 pagesSymptoms of CvsstudymedicNo ratings yet
- The Arterial PulseDocument22 pagesThe Arterial PulsestudymedicNo ratings yet
- Skills 2Document22 pagesSkills 2studymedicNo ratings yet
- Measles (Rubeola) VirusDocument16 pagesMeasles (Rubeola) Virusstudymedic100% (1)
- Inspection and Palpation of The HeartDocument38 pagesInspection and Palpation of The Heartstudymedic100% (2)
- General Examination For CVSDocument29 pagesGeneral Examination For CVSstudymedic100% (1)
- Blood PressureDocument11 pagesBlood PressurestudymedicNo ratings yet
- Pathology Practical Exam Study SheetDocument4 pagesPathology Practical Exam Study SheetstudymedicNo ratings yet
- Mumps VirusDocument15 pagesMumps Virusstudymedic0% (1)
- Paramyxoviridae EditedDocument30 pagesParamyxoviridae EditedstudymedicNo ratings yet
- Main Features of ParamyxovirusesDocument7 pagesMain Features of ParamyxovirusesstudymedicNo ratings yet
- Laboratory Diagnosis of Viral InfectionDocument37 pagesLaboratory Diagnosis of Viral InfectionstudymedicNo ratings yet
- Antihyperlipidaemic DrugsDocument44 pagesAntihyperlipidaemic DrugsstudymedicNo ratings yet
- Rhino VirusesDocument20 pagesRhino VirusesstudymedicNo ratings yet
- Corona VirusesDocument42 pagesCorona VirusesstudymedicNo ratings yet
- Adenoviruses AdenovirusesDocument25 pagesAdenoviruses AdenovirusesstudymedicNo ratings yet
- Practical Microbiology 2nd YearDocument33 pagesPractical Microbiology 2nd Yearstudymedic100% (1)
- Orthomyxoviruses Orthomyxoviruses Influenza Viruses Influenza VirusesDocument44 pagesOrthomyxoviruses Orthomyxoviruses Influenza Viruses Influenza VirusesstudymedicNo ratings yet
- Culture Media NoteDocument5 pagesCulture Media Notestudymedic100% (1)
- Responsi Stemi Dr. Tuko SP - JP FixDocument56 pagesResponsi Stemi Dr. Tuko SP - JP FixcintaNo ratings yet
- Definition, Presentation, Treatment, and Histology: by Dr. Martin Mihm, Jr. and Linda Rozell-Shannon, M.SDocument17 pagesDefinition, Presentation, Treatment, and Histology: by Dr. Martin Mihm, Jr. and Linda Rozell-Shannon, M.SAriandindi AriandiNo ratings yet
- Coronary Artery Bypass Graft Cabg SurgeryDocument26 pagesCoronary Artery Bypass Graft Cabg SurgeryNogra CarlNo ratings yet
- 1 4927329208029413644 PDFDocument578 pages1 4927329208029413644 PDFWaseem UllahNo ratings yet
- (The European Society of Cardiology Series) Jose Luis Zamorano, Jeroen Bax, Juhani Knuuti, Patrizio Lancellotti, Fausto Pinto, Bogdan A. Popescu, Udo Sechtem - The ESC Textbook of Cardiovascular ImagiDocument865 pages(The European Society of Cardiology Series) Jose Luis Zamorano, Jeroen Bax, Juhani Knuuti, Patrizio Lancellotti, Fausto Pinto, Bogdan A. Popescu, Udo Sechtem - The ESC Textbook of Cardiovascular ImagiEdu MartinsNo ratings yet
- Massive Pulmonary EmbolismDocument3 pagesMassive Pulmonary Embolismnananana123No ratings yet
- Cardiac CycleDocument2 pagesCardiac CycleU Than HanNo ratings yet
- Deborah Mukendenge Mujinga Nurs201Document6 pagesDeborah Mukendenge Mujinga Nurs201Lois MpangaNo ratings yet
- Hypertensive Crisis: Haerani Rasyid Hasanuddin University MakassarDocument47 pagesHypertensive Crisis: Haerani Rasyid Hasanuddin University MakassarVictor PratamaNo ratings yet
- Hypertensive RetinopathyDocument32 pagesHypertensive Retinopathyณัช เกษม100% (7)
- Vasculitele Anca Pozitive: O Privire Generală: Monica Copotoiu, MD, PHDDocument63 pagesVasculitele Anca Pozitive: O Privire Generală: Monica Copotoiu, MD, PHDMaria CoroiuNo ratings yet
- Cardiovascular System AnatomyDocument13 pagesCardiovascular System AnatomyDwi Junita SariNo ratings yet
- Sample ReportDocument3 pagesSample ReportRobeants Charles PierreNo ratings yet
- Statin Treatment and Stroke Outcome in The StrokeDocument7 pagesStatin Treatment and Stroke Outcome in The StrokeAnnafiatu zakiahNo ratings yet
- Scorebuilders Cardiac ReviewDocument16 pagesScorebuilders Cardiac Reviewboogie33100% (1)
- Ischemic Heart DiseaseDocument31 pagesIschemic Heart DiseaseRohit SahNo ratings yet
- Pulmonary Hypertension: Annals of Internal MedicinetDocument16 pagesPulmonary Hypertension: Annals of Internal MedicinetAlicia TGNo ratings yet
- Coronarry Artery DiseaseDocument24 pagesCoronarry Artery DiseaseAriess897No ratings yet
- CobaDocument58 pagesCobakompleks comedyNo ratings yet
- Bio Lab 11Document5 pagesBio Lab 11Sarah JaglalNo ratings yet
- Vastarel MR From Decades of Clinical Experience inDocument6 pagesVastarel MR From Decades of Clinical Experience inJonathan Ian ArinsolNo ratings yet
- Vital SignDocument40 pagesVital SignYoelBagusGiarto0% (1)
- Concept Evaluation and Future Perspectives of PERKAT RV - A Novel Right Ventricular Assisit DeviceDocument5 pagesConcept Evaluation and Future Perspectives of PERKAT RV - A Novel Right Ventricular Assisit DeviceYEZINo ratings yet
- CTO GuideDocument14 pagesCTO GuideTeodor BicaNo ratings yet
- MCQ Internal Medicine PDFDocument448 pagesMCQ Internal Medicine PDFAyaa Yousef100% (5)
- Kami Export - CirculatorySystem12052022Document1 pageKami Export - CirculatorySystem12052022Nyla ScottNo ratings yet
- Clinical Suspicion of Left Ventricular Apical Thrombus - What To Do?: A Case ReportDocument11 pagesClinical Suspicion of Left Ventricular Apical Thrombus - What To Do?: A Case ReportIJAR JOURNALNo ratings yet
- Understanding the Cardiac CycleDocument49 pagesUnderstanding the Cardiac CycleJardee Datsima100% (1)
- Ehaa575 Supplementary DataDocument35 pagesEhaa575 Supplementary DataDaniela Zuluaga HurtadoNo ratings yet
- CVADocument22 pagesCVAPankaj Shahi100% (1)