You might also like
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Support StaffDocument1 pageSupport Staffapi-267659754No ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- 1mk Summer Contact InformationDocument1 page1mk Summer Contact Informationapi-267659754No ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- WWPT Home Learning Project 2015Document1 pageWWPT Home Learning Project 2015api-234959883No ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Morning Announcement For Out of Uniform DayDocument2 pagesMorning Announcement For Out of Uniform Dayapi-267659754No ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Art AuctionDocument1 pageArt Auctionapi-267659754No ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
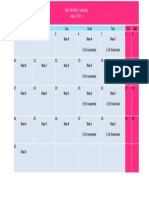
- May CalendarDocument1 pageMay Calendarapi-267659754No ratings yet
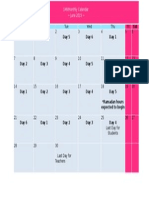
- June Calendar v2Document1 pageJune Calendar v2api-267659754No ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Book FairDocument1 pageBook Fairapi-267659754No ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Home LearningDocument5 pagesHome Learningapi-267659754No ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Health QuestionaireDocument1 pageHealth Questionaireapi-267659754No ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- Change Initiative Trip April 23Document1 pageChange Initiative Trip April 23api-267659754No ratings yet
- SLC Parent ReflectionDocument1 pageSLC Parent Reflectionapi-267659754No ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- 3d ShapesDocument2 pages3d Shapesapi-267659754No ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Home Learning Project WwaDocument5 pagesHome Learning Project Wwaapi-267659754No ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Parent Teacher ConferenceDocument1 pageParent Teacher Conferenceapi-267659754No ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- ASSIGNMENTDocument5 pagesASSIGNMENTPanchdev KumarNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- GII-07 Training MaterialDocument191 pagesGII-07 Training MaterialIris Amati MartinsNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Ashe v. Swenson, 397 U.S. 436 (1970)Document25 pagesAshe v. Swenson, 397 U.S. 436 (1970)Scribd Government DocsNo ratings yet
- Banking & Finance Awareness 2016 (Jan-Nov) by AffairsCloudDocument167 pagesBanking & Finance Awareness 2016 (Jan-Nov) by AffairsCloudkaushikyNo ratings yet
- CQI - Channel Quality Indicator - Ytd2525Document4 pagesCQI - Channel Quality Indicator - Ytd2525TonzayNo ratings yet
- Testing Your Understanding: The Dash, Slash, Ellipses & BracketsDocument2 pagesTesting Your Understanding: The Dash, Slash, Ellipses & BracketsBatsaikhan DashdondogNo ratings yet
- ArenavirusDocument29 pagesArenavirusRamirez GiovarNo ratings yet
- School For Good and EvilDocument4 pagesSchool For Good and EvilHaizyn RizoNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Louis Theroux PowerpointDocument6 pagesLouis Theroux Powerpointapi-330762792No ratings yet
- Al-Rimawi Et Al-2019-Clinical Oral Implants ResearchDocument7 pagesAl-Rimawi Et Al-2019-Clinical Oral Implants ResearchSohaib ShujaatNo ratings yet
- Phantom Susan KayDocument379 pagesPhantom Susan Kaytheeyeofthemoon100% (9)
- 7 Years - Lukas Graham SBJDocument2 pages7 Years - Lukas Graham SBJScowshNo ratings yet
- People v. Cresencia ReyesDocument7 pagesPeople v. Cresencia ReyesAnggling DecolongonNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Jolly Phonics Teaching Reading and WritingDocument6 pagesJolly Phonics Teaching Reading and Writingmarcela33j5086100% (1)
- Formula Sheet For Astronomy 1 - Paper 1 and Stars & PlanetsDocument2 pagesFormula Sheet For Astronomy 1 - Paper 1 and Stars & PlanetsprashinNo ratings yet
- Mil HDBK 1390 PDFDocument31 pagesMil HDBK 1390 PDFsleepanon4362No ratings yet
- 4 Reasons To Walk With GodDocument2 pages4 Reasons To Walk With GodNoel Kerr CanedaNo ratings yet
- The Story of Babri MasjidDocument54 pagesThe Story of Babri MasjidKiran Penumala100% (1)
- APCHG 2019 ProceedingsDocument69 pagesAPCHG 2019 ProceedingsEnrico SocoNo ratings yet
- Numl Lahore Campus Break Up of Fee (From 1St To 8Th Semester) Spring-Fall 2016Document1 pageNuml Lahore Campus Break Up of Fee (From 1St To 8Th Semester) Spring-Fall 2016sajeeNo ratings yet
- Javier Couso, Alexandra Huneeus, Rachel Sieder Cultures of Legality Judicialization and Political Activism in Latin America Cambridge Studies in Law and SocietyDocument290 pagesJavier Couso, Alexandra Huneeus, Rachel Sieder Cultures of Legality Judicialization and Political Activism in Latin America Cambridge Studies in Law and SocietyLívia de SouzaNo ratings yet
- The Republic of LOMAR Sovereignty and International LawDocument13 pagesThe Republic of LOMAR Sovereignty and International LawRoyalHouseofRA UruguayNo ratings yet
- The Pantheon of Greek Gods and GoddessesDocument2 pagesThe Pantheon of Greek Gods and Goddessesapi-226457456No ratings yet
- Vadiyanatha AstakamDocument4 pagesVadiyanatha AstakamRaga MalikaNo ratings yet
- Comic Conversations – Lesson Plan & TemplatesDocument15 pagesComic Conversations – Lesson Plan & TemplatesShengdee OteroNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Test Unit 3Document2 pagesTest Unit 3RAMONA SECUNo ratings yet
- Kung Fu MedicinesDocument9 pagesKung Fu MedicinesDavid HewittNo ratings yet
- PHILIPPINE INCOME TAX REVIEWERDocument99 pagesPHILIPPINE INCOME TAX REVIEWERquedan_socotNo ratings yet
- Contemporary Philippine Arts From The RegionsDocument29 pagesContemporary Philippine Arts From The RegionsDina Ilagan50% (2)
- Chapter 11, 12 Curve Tracing and EnvelopeDocument37 pagesChapter 11, 12 Curve Tracing and EnvelopeNitish PokhrelNo ratings yet
- The HPV Vaccine On Trial: Seeking Justice For A Generation BetrayedFrom EverandThe HPV Vaccine On Trial: Seeking Justice For A Generation BetrayedRating: 4.5 out of 5 stars4.5/5 (13)
- Do You Believe in Magic?: The Sense and Nonsense of Alternative MedicineFrom EverandDo You Believe in Magic?: The Sense and Nonsense of Alternative MedicineNo ratings yet