You might also like
- Cardiac Action Potential - WikipediaDocument67 pagesCardiac Action Potential - WikipediaMohd. Mudabbir-Ul- IslamNo ratings yet
- Respiratory System: A Tutorial Study GuideFrom EverandRespiratory System: A Tutorial Study GuideRating: 5 out of 5 stars5/5 (1)
- Atrial Systole: The End of DiastoleDocument9 pagesAtrial Systole: The End of DiastoleSophia MahboobNo ratings yet
- Frank-Starling LawDocument6 pagesFrank-Starling LawGauri RastogiNo ratings yet
- Basic Arrythmias: Prof. Maximin A. Pomperada, RN, MNDocument70 pagesBasic Arrythmias: Prof. Maximin A. Pomperada, RN, MNRellie CastroNo ratings yet
- Cardiac Arrhythmia: Prepared By: Charina Gail O. Baloy, RPH, Msc. (C.)Document44 pagesCardiac Arrhythmia: Prepared By: Charina Gail O. Baloy, RPH, Msc. (C.)Chinenye Akwue100% (1)
- HANDOUTS-Non Invasive VentilationDocument15 pagesHANDOUTS-Non Invasive VentilationKristine MangasepNo ratings yet
- Gas Transport PDFDocument19 pagesGas Transport PDFMarilia BonorinoNo ratings yet
- Action Potential ECGDocument11 pagesAction Potential ECGAndrei ManeaNo ratings yet
- Notes in Physiology 2nd PDFDocument37 pagesNotes in Physiology 2nd PDFDany SamuelNo ratings yet
- Tough Love With Bell HooksDocument6 pagesTough Love With Bell HooksGil Frank100% (1)
- Hyperkalemia and HypokalemiaDocument37 pagesHyperkalemia and HypokalemiaDiena AshlihatiNo ratings yet
- Progenitor Heart Cells Lie in The Epiblast, Immediately Adjacent To TheDocument15 pagesProgenitor Heart Cells Lie in The Epiblast, Immediately Adjacent To TheJehangir AllamNo ratings yet
- The Coronary CirculationDocument12 pagesThe Coronary CirculationJulia PutnikNo ratings yet
- Anatomy and Physiology Ii SMS 1224: Norhayati Ismail NOV 2011Document50 pagesAnatomy and Physiology Ii SMS 1224: Norhayati Ismail NOV 2011Shirley LourdesNo ratings yet
- Physiology Lecture 10 Q-Bank (Cardiac Muscle - Action Potentials)Document15 pagesPhysiology Lecture 10 Q-Bank (Cardiac Muscle - Action Potentials)ChrisOrtNo ratings yet
- Coronary CirculationDocument47 pagesCoronary CirculationSuresh KumarNo ratings yet
- By: Calaour, Carrey Dasco, Danica Amor Dimatulac, Kevin Lim, Shiela Marie Pagulayan, Sheena May Pua, Mar KristineDocument41 pagesBy: Calaour, Carrey Dasco, Danica Amor Dimatulac, Kevin Lim, Shiela Marie Pagulayan, Sheena May Pua, Mar Kristineceudmd3d100% (2)
- Arrhythmia S: DRDM KillingoDocument95 pagesArrhythmia S: DRDM KillingoMalueth Angui100% (1)
- The Cardiac Cycle: Chapter 19Document62 pagesThe Cardiac Cycle: Chapter 19BishwambherNo ratings yet
- Cardiac Cycle: Mechanical Event and Their Electrical and Clinical CorrelationDocument28 pagesCardiac Cycle: Mechanical Event and Their Electrical and Clinical Correlationhawas muhammed100% (1)
- The Circulatory System BookletDocument30 pagesThe Circulatory System BookletTroy CampbellNo ratings yet
- I.V Fluid: PathologyDocument7 pagesI.V Fluid: PathologyruchikaNo ratings yet
- Cardio Vascular SystemDocument22 pagesCardio Vascular SystemdeborahNo ratings yet
- Action Potential of Cardiac MusclesDocument16 pagesAction Potential of Cardiac Muscleswaqas_xsNo ratings yet
- Cardiovascular Blood VesselsDocument12 pagesCardiovascular Blood VesselswatuwaitingforNo ratings yet
- Nur 111 Session 6 Sas 1Document12 pagesNur 111 Session 6 Sas 1Zzimply Tri Sha UmaliNo ratings yet
- Ks Module 12Document29 pagesKs Module 12jerinthomasrajanNo ratings yet
- Oxygen Dissociation CurvesDocument11 pagesOxygen Dissociation CurvesSajin Sali75% (4)
- Heart Muscle: The Heart As A Pump and FunctionDocument4 pagesHeart Muscle: The Heart As A Pump and Functionmcwnotes100% (1)
- Cardiac Cycle by Bala GoyalDocument14 pagesCardiac Cycle by Bala Goyaltee su lingNo ratings yet
- Heart Sounds - PracticalDocument7 pagesHeart Sounds - Practicalshadapaaak100% (1)
- Cardiac CycleDocument12 pagesCardiac Cycleanupam manu100% (1)
- 05 Cardiovascular System PhysiologyDocument34 pages05 Cardiovascular System PhysiologyKaye Alyssa EnriquezNo ratings yet
- Lec-6) STsegment in MIDocument44 pagesLec-6) STsegment in MISaeed Shah100% (1)
- Cardiac OutputDocument61 pagesCardiac OutputSyed Ali MoosaNo ratings yet
- Describe The Factors Affecting Cardiac OutputDocument6 pagesDescribe The Factors Affecting Cardiac OutputSis SukarnoNo ratings yet
- Intravenous FluidsDocument19 pagesIntravenous Fluidsblack pink in ur area 21100% (1)
- Heart Failure RevisionDocument4 pagesHeart Failure RevisionBlanaid MargaretNo ratings yet
- Respiratory SystemDocument36 pagesRespiratory SystemPritha Bhuwapaksophon100% (1)
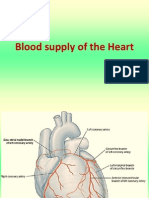
- Blood Supply of HeartDocument7 pagesBlood Supply of Heartmariposa_0612No ratings yet
- Myocardial Infarction MIDocument23 pagesMyocardial Infarction MIأبو محمدNo ratings yet
- ... 4 Finals Cardiovascular PhysiologyDocument8 pages... 4 Finals Cardiovascular PhysiologyELIZABETH GRACE AMADORNo ratings yet
- Autonomic Nervous SystemDocument50 pagesAutonomic Nervous SystemEbti Rizki UtamiNo ratings yet
- Chapter 11-The Normal ElectrocardiogramDocument18 pagesChapter 11-The Normal Electrocardiogrammuna s100% (1)
- Cardiac Cycle: Prepared By: Mineshkumar Prajapati Roll No: 05 Biomedical Science (2021-22)Document21 pagesCardiac Cycle: Prepared By: Mineshkumar Prajapati Roll No: 05 Biomedical Science (2021-22)minesh prajapatiNo ratings yet
- Lung Protective Mechanical Ventilation StrategiesDocument4 pagesLung Protective Mechanical Ventilation StrategiesAnne Julia AgustinNo ratings yet
- Examination of Cardiovascular SystemDocument24 pagesExamination of Cardiovascular SystemThilak JayalathNo ratings yet
- ANPH-M2-CU8. The HeartDocument20 pagesANPH-M2-CU8. The HeartMary Grace MapulaNo ratings yet
- 3rd Lecture On Nerve Physiology by Dr. RoomiDocument12 pages3rd Lecture On Nerve Physiology by Dr. RoomiMudassar RoomiNo ratings yet
- Cardiac Output and Hemodynamic MeasurementDocument29 pagesCardiac Output and Hemodynamic Measurementdeepa100% (1)
- The MyocardiumDocument8 pagesThe MyocardiumKyrene San Pedro RosalesNo ratings yet
- Composition and Function of Blood ComponentsDocument17 pagesComposition and Function of Blood ComponentsPrakash Kumar Nayak100% (1)
- Physiology of Heart in DetailDocument101 pagesPhysiology of Heart in Detailakanksha sharmaNo ratings yet
- Anesthesia Cheat Sheet: Dogs CatsDocument3 pagesAnesthesia Cheat Sheet: Dogs CatsJoão Pedro Pereira100% (1)
- NCM 103-Cardio Anatomy & PhysioDocument56 pagesNCM 103-Cardio Anatomy & Physiolouradel100% (1)
- Cardiovascular System: More Than Just The HeartDocument34 pagesCardiovascular System: More Than Just The HearteliseudesafateNo ratings yet
- Regulation of Heart Rate, Stroke Volume, Cardiac Output, Blood FlowDocument20 pagesRegulation of Heart Rate, Stroke Volume, Cardiac Output, Blood FlowShveta MahajanNo ratings yet
- USMLE Preparation LinksDocument1 pageUSMLE Preparation Linksselvakumar.anbalagan100% (1)
- Print Materials For Step1Document2 pagesPrint Materials For Step1kowaikowarNo ratings yet
- Quick Ekg ReferenceDocument23 pagesQuick Ekg Referencekowaikowar100% (2)
- CELL TYPES of The NERVOUS SYSTEM (Action Potential N Membrane Potential)Document3 pagesCELL TYPES of The NERVOUS SYSTEM (Action Potential N Membrane Potential)kowaikowarNo ratings yet
- Case For ECG... 1Document2 pagesCase For ECG... 1kowaikowarNo ratings yet
- Lateral Pharyngeal Region (Carotid Artery)Document5 pagesLateral Pharyngeal Region (Carotid Artery)kowaikowarNo ratings yet
- Magnetic Resonance Imaging - 2013 - Jung - Spin Echo Magnetic Resonance ImagingDocument13 pagesMagnetic Resonance Imaging - 2013 - Jung - Spin Echo Magnetic Resonance ImagingMSNo ratings yet
- Chapter 2 Geometry of CrystalsDocument56 pagesChapter 2 Geometry of CrystalssfdafNo ratings yet
- Presen V.Prem: Ted by PrasadDocument46 pagesPresen V.Prem: Ted by PrasadAshutosh SharmaNo ratings yet
- Nihms 56748Document35 pagesNihms 56748burcuu34No ratings yet
- Chapter 21 Intro To CNS PharmaDocument8 pagesChapter 21 Intro To CNS PharmaChristine Annmarie TapawanNo ratings yet
- SAED in TEMDocument13 pagesSAED in TEMbishnukoiry0% (1)
- Protein DenaturationDocument17 pagesProtein DenaturationSubir DasNo ratings yet
- Cell Structures and Their FunctionsDocument2 pagesCell Structures and Their FunctionsSheikha KamidNo ratings yet
- Experiemnt 1 Carine May31Document22 pagesExperiemnt 1 Carine May31Mirtunjay KumarNo ratings yet
- Assignment 5 Protein Localization Prediction of Protein StructureDocument2 pagesAssignment 5 Protein Localization Prediction of Protein StructureViệt Lê Nguyễn HoàngNo ratings yet
- Transport Across Cell MembraneDocument20 pagesTransport Across Cell Membrane安 娜 胡No ratings yet
- Cell Structure and FunctionDocument66 pagesCell Structure and FunctionMark Anthony CorpuzNo ratings yet
- Crystal MorphologyDocument41 pagesCrystal Morphologyagvega69109No ratings yet
- MODULE 1.3 Cell Membrane TransportDocument11 pagesMODULE 1.3 Cell Membrane TransportBrandon James SevillaNo ratings yet
- Chapter 3 Antigen and AntibodyDocument41 pagesChapter 3 Antigen and AntibodyDaarshiny ElumalaiNo ratings yet
- Biochemistry Study Notes PDFDocument5 pagesBiochemistry Study Notes PDFLofiSophicalNo ratings yet
- NCRP - 151 - RAyos X Infraestructura PDFDocument35 pagesNCRP - 151 - RAyos X Infraestructura PDFmeliclau10% (1)
- Solids JEE NEET PDFDocument12 pagesSolids JEE NEET PDFArpit RawatNo ratings yet
- Lecture 6 - Cell Membranes and TransportDocument42 pagesLecture 6 - Cell Membranes and TransportGloria LiNo ratings yet
- Protein Engineering Syllabus BIA1014Document1 pageProtein Engineering Syllabus BIA1014Dhanalakshmi SaravananNo ratings yet
- Cell Transport Mechanism WorksheetDocument2 pagesCell Transport Mechanism WorksheetMay VicenteNo ratings yet
- Introduction To Cell Biology PDFDocument41 pagesIntroduction To Cell Biology PDFediaz_956003100% (2)
- Tugas 1 Advanced CrystallographyDocument7 pagesTugas 1 Advanced CrystallographyMuhammad Hisyam FMIPANo ratings yet
- UntitledDocument339 pagesUntitledJOS� FRANCISCO G�MEZ RODR�GUEZNo ratings yet
- Lecture 2 - CML 231 - Atomic Bonding and Structure of SolidsDocument115 pagesLecture 2 - CML 231 - Atomic Bonding and Structure of SolidsTony StarkNo ratings yet
- Crystal Lattices and Unit CellsDocument8 pagesCrystal Lattices and Unit CellsAnshika SinghNo ratings yet
- The Cell: By: Kinza ChaudhariDocument16 pagesThe Cell: By: Kinza ChaudhariChris GayleNo ratings yet
- Chap 3 Movement of Substances Across A Plasma MembraneDocument18 pagesChap 3 Movement of Substances Across A Plasma MembraneNURIN BISHARAH BINTI MOHAMAD SHAHRUNNIZAM MoeNo ratings yet
- Unit 2 ReviewerDocument4 pagesUnit 2 Revieweraaleah moscaNo ratings yet
- Rigaku Journal 32-2-35-43Document9 pagesRigaku Journal 32-2-35-43Acácio CruzNo ratings yet
- How to Teach Nature Journaling: Curiosity, Wonder, AttentionFrom EverandHow to Teach Nature Journaling: Curiosity, Wonder, AttentionRating: 4.5 out of 5 stars4.5/5 (3)
- A-level Biology Revision: Cheeky Revision ShortcutsFrom EverandA-level Biology Revision: Cheeky Revision ShortcutsRating: 5 out of 5 stars5/5 (5)
- Quantum Physics for Beginners: Simple Illustrated Guide to Discover with Practical Explanations the Paradoxes of the Life and Universe Reconsidering RealityFrom EverandQuantum Physics for Beginners: Simple Illustrated Guide to Discover with Practical Explanations the Paradoxes of the Life and Universe Reconsidering RealityRating: 2 out of 5 stars2/5 (1)
- Lower Secondary Science Workbook: Stage 8From EverandLower Secondary Science Workbook: Stage 8Rating: 5 out of 5 stars5/5 (1)
- Interactive Science Notebook: The Human Body WorkbookFrom EverandInteractive Science Notebook: The Human Body WorkbookRating: 4 out of 5 stars4/5 (2)
- STEM Labs for Physical Science, Grades 6 - 8From EverandSTEM Labs for Physical Science, Grades 6 - 8Rating: 3.5 out of 5 stars3.5/5 (6)
- How Do Cell Phones Work? Technology Book for Kids | Children's How Things Work BooksFrom EverandHow Do Cell Phones Work? Technology Book for Kids | Children's How Things Work BooksNo ratings yet
- Nature-Based Learning for Young Children: Anytime, Anywhere, on Any BudgetFrom EverandNature-Based Learning for Young Children: Anytime, Anywhere, on Any BudgetRating: 5 out of 5 stars5/5 (1)
- The Periodic Table of Elements - Post-Transition Metals, Metalloids and Nonmetals | Children's Chemistry BookFrom EverandThe Periodic Table of Elements - Post-Transition Metals, Metalloids and Nonmetals | Children's Chemistry BookNo ratings yet
- Interactive Notebook: Life Science, Grades 5 - 8From EverandInteractive Notebook: Life Science, Grades 5 - 8Rating: 5 out of 5 stars5/5 (4)
- Nature Preschools and Forest Kindergartens: The Handbook for Outdoor LearningFrom EverandNature Preschools and Forest Kindergartens: The Handbook for Outdoor LearningRating: 3.5 out of 5 stars3.5/5 (3)
- Airplane Flying Handbook: FAA-H-8083-3C (2024)From EverandAirplane Flying Handbook: FAA-H-8083-3C (2024)Rating: 4 out of 5 stars4/5 (12)
- The Periodic Table of Elements - Alkali Metals, Alkaline Earth Metals and Transition Metals | Children's Chemistry BookFrom EverandThe Periodic Table of Elements - Alkali Metals, Alkaline Earth Metals and Transition Metals | Children's Chemistry BookNo ratings yet
- A-Level Chemistry Revision: Cheeky Revision ShortcutsFrom EverandA-Level Chemistry Revision: Cheeky Revision ShortcutsRating: 4 out of 5 stars4/5 (5)