NURSING CARE PLAN NAME OF STUDENT: NAME OF CLIENT: xxx DIAGNOSIS OR CLINICAL IMPRESSION: Pancreatic mass probabaly malignant
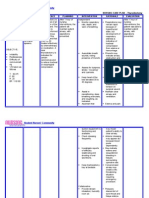
CUES S: * Female * 62 years old * Post-operative patient (Operation: March 23, 2010) * Masakit yung kanang kamay ko kasi mali ata yung pagkakasaksak nung IV. Sumasakit 'yung sutures kasi. O: *(+) palpable mass liver edge 4 cm below RCM * Normal Weight BMI = 20.76 Height: 170 cm. Weight: 60 kg. * Vital signs: (Mar. 29, 2010) RR = 24/min Temp. = 37.6 C P = 64/min BP = 120/60 *Latest hematology results: (March 21, 2010) Decreased RBC, Hgb and Hct. RBC = 2.93 x 10 ^12/L NURSING DIAGNOSIS Risk for Infection related to compromised host defenses secondary to probable pancreatic cancer BACKGROUND KNOWLEDGE Medical factors predisposing to infection include: immunocompromised: steroids, immunosuppressants, AIDS, connective tissue disease, cancer or leukaemia, chemotherapy (very dangerous as signs diminished) previous infection: rheumatic fever, TB or jaundice surgical conditions: gallstones, diverticular disease, prostatism and prolapse recent surgery or procedure, dentistry and minor injury family history or other close contact of infection medication including selfmedication and blood products malnourished GOALS AND OBJECTIVES GOAL: At the end of the nursing intervention, Mrs. xxx will remain infection-free and report risk factors associated with infection and precautions needed. OBJECTIVES: After the nursing intervention, xxx will: 1. Describe 2 methods of transmission of infection. 2. Verbalize understanding of individual/causative risk factors in her own words. 3. Describe the influence of nutrition on prevention of infection in her own words. 4. Maintain adequate hydration. 5. Demonstrate meticulous hand washing procedure. 6. Perform preoperative body shower or scrubs when indicated. 7. Demonstrate proper deep breathing exercises, coughing technique and ROM exercises.
DATE OF ASSIGNMENT: March 22, 2010 CIVIL STATUS: Separated AGE: 62 SEX: F WARD: 4 BED: 2 NURSING INTERVENTIONS AND RATIONALE The student nurse will: 1.Instruct the client about the various modes of transmission of microorganisms and risk factors. R: This is done to prevent the spread of microorganisms. 2. Enumerate to the individual and family members the signs and symptoms of infection. R: This is done for the client to be able to assess herself for possible infection and inform the nearest health professional and be given immediate care. 3. Encourage and maintain caloric and protein intake in diet in accordance with prescribed soft diet. R: This is done to strengthen the immunity without compromising the prescribed diet. 4. Inform the client about the importance of maintaining adequate hydration. R: Adequate hydration helps in regulating the body temperature and removing excess wastes and toxins. 5. Inform and demonstrate to the client, the proper hand washing technique and procedure. EVALUATION By the end of the nursing intervention, Ms. xxx will able to: 1. Accurately describe 2 methods of transmission of infection. 2. Verbalize understanding of individual/causative risk factors in her own words. 3. Describe the influence of nutrition on prevention of infection in her own words. 4. Maintain adequate hydration. 5. Properly demonstrate meticulous hand washing procedure. 6. Perform preoperative body shower or scrubs when indicated. 7. Demonstrate proper deep breathing exercises, coughing technique and ROM exercises.
SOURCE: http://www.gpnotebook.co.uk /simplepage.cfm? ID=1543897156 Nosocomial infection is an infection caught while hospitalized. Most nosocomial infections are due to bacteria. Since antibiotics are frequently used within hospitals, the types of bacteria and their resistance to antibiotics is different than bacteria outside of the hospital. Nosocomial infections can be
Hgb: 98 g/L HCT: 0.292 Increased Neutrophils and WBC. Neutrophils = 0.896 WBC = 12.10 10^9/L *Antibiotic Therapy (Metronidazole 1cap TID x 2 days) * NSS infused at 31 gtts at right arm, (+) inflammation
serious and difficult to treat. SOURCE: http://www.medterms.com/script /main/art.asp?articlekey=10430
R: Good hand washing is the first line of defense against the spread of many illnesses. 6. Perform/instruct in preoperative body shower/scrubs when indicated. R: This is done to empower the client with knowledge about what are effective ways to prevent infection. Preoperative body showers are done to maintain cleanliness of patient before operation. 7. Encourage early ambulation, deep breathing, coughing, position change. R: This is done for the mobilization of respiratory secretions.
S: Medyo kinakabahan siyempre. I think that is normal. We do not know what to expect. I just use prayers to calm down. Client cried when the nun said that she could not administer the holy sacrament the day of her surgery. O: BP = 120/60 RR = 24/min PR = 64/min (+) sleep
Anxiety (moderate) related to actual or perceived threat to biologic integrity secondary to invasive procedures
Anxiety is a state of mental uneasiness, apprehension, dread, or foreboding or a feeling of helplessness related to an impending or anticipated unidentified threat to self or significant relationships.
GOAL: At the end of the nursing intervention, Mrs. Xxx will relate an increase in psychological and physiologic comfort. OBJECTIVES: After the nursing intervention, Mrs. Xxx will: 1. Explain the importance of preoperative laboratory tests in her own words. 2. Verbalize understanding of bowel and skin preparation and need to remove all makeup and jewelry prior to surgery. 3. State her own understanding of the procedure to be done and
The student nurse will: 1. Explain the need for preoperative laboratory tests R: The more information a client has, the more she is reassured. 2. Discuss bowel and skin preparation and the need to remove all jewelry, nail polish, make-up, etc. prior to surgery. R: Discuss preparations to empower client. 3. Briefly discuss the procedure to be done and what the client could expect from it. R: The more information a client has, the more she is reassured.
After the nursing intervention, Ms. xxx will: 1. Explain the importance of preoperative laboratory tests in her own words. 2. Verbalize understanding of bowel and skin preparation and need to remove all make-up and jewelry prior to surgery. 3. State her own understanding of the procedure to be done and what could be expected 4. State the need for restriction food and oral fluids for at least 8
Anxiety on the unkniwn, especially surgery, is natural and common. Moderate pain increases in the arousal state to a point where the person expresses feelings of tensions, nervousness or concern. SOURCE:
Kozier, B., Erb, G., Berman, A. & Snyder, S. (2004). Fundamentals of nursing (7th ed). Philippines:
disturbances, weakness, faintness, fatigue Gastroscopy results: Postendoscopic diagnosis: duodenal mass probably malignant, 1 VS infiltration, hiatal hernia S: * Female * 62 years old * Post-operative patient (Operation: March 23, 2010) * Masakit yung kanang kamay ko kasi mali ata yung pagkakasaksak nung IV. Sumasakit 'yung sutures kasi. Pain rating for pain in sutures: 5 O: *(+) palpable mass liver edge 4 cm below RCM * Vital signs: (Mar. 29, 2010) RR = 24/min Temp. = 37.6 C P = 64/min BP = 120/60 *Latest Acute Pain related to tissue trauma secondary to surgery
Pearson Prentice Hall
what could be expected 4. State the need for restriction food and oral fluids for at least 8 hours prior to surgery. 5. Demonstrate ambulation, leg exercises, deep breathing and coughing exercises.
4. Explain the need for restriction of food and oral fluids for at least 8hours prior to surgery. R: The more information a client has, the more she is reassured. 5. Demonstrate the need for ambulation, leg exercises, deep breathing and coughing exercises. R: This are nonpharmacological methods used to lessen anxiety. 1. Explain causes of pain to the person, if known. R: The more information a client has, the more she is reassured. 2. Relate how long the pain may last. R: The more information a client has, the more she is reassured. 3. Explain diagnostic procedures and tests in detail by relating discomforts and sensations that will be felt. R: The more information a client has, the more she is reassured. 4. Discuss the reasons why an individual may experience increased or decreased pain (fatigue, or presence of distractions). R: The more information a client has, the more she is reassured. 5. Encourage family support and to to give attention also when pain is not exhibited. R: Family support increases
hours prior to surgery. 5. Demonstrate ambulation, leg exercises, deep breathing and coughing exercises.
Pain is an unpleasant and highly personal experience that may be imperceptible to others, while consuming all parts of the person's life.
Goal: After nursing intervention, Mrs. Xxx will relate relief after a satisfactory relief measure. Objectives: After nursing intervention, Mrs. Xxx will: 1. Explain causes of pain to the person, if known. 2. Relate how long the pain may last. 3. State her own understanding of procedure and give discomforts and sensations that will be felt. 4. State reasons why an individual may experience increased or decreased pain (fatigue, or presence of distractions) 5. Verbalize increase of relief with family support 6. Rest during the day and have uninterrupted sleep at night 7. Select and use a method of distraction during acute pain.
After nursing intervention, Mrs. Xxx will: 1. Explain causes of pain to the person, if known. 2. Relate how long the pain may last. 3. State her own understanding of procedure and give discomforts and sensations that will be felt. 4. State reasons why an individual may experience increased or decreased pain (fatigue, or presence of distractions) 5. Verbalize increase of relief with family support 6. Rest during the day and have uninterrupted sleep at night 7. Select and use a method of distraction
Pain is a physical and emotional experience.
Effective pain management is an important aspect of nursing care to promote healing, prevent complications, reuce suffering and prevent the development of incurable pain states.
Visceral pain is pain arising from organs or hollow viscera.
Source:
Kozier, B., Erb, G., Berman, A. & Snyder, S. (2004). Fundamentals of nursing (7th ed). Philippines: Pearson Prentice Hall
hematology results: (March 21, 2010) Decreased RBC, Hgb and Hct. RBC = 2.93 x 10 ^12/L Hgb: 98 g/L HCT: 0.292 Increased Neutrophils and WBC. Neutrophils = 0.896 WBC = 12.10 10^9/L *Antibiotic Therapy (Metronidazole 1cap TID x 2 days) * NSS infused at 31 gtts at right arm, (+) inflammation
reassurance of patient. 8. Select and use non-invasive pain-relief measures. (relaxation techniques, music therapy, moment of discussion) 6. Provide person with opportunities to rest during the day and with periods of uninterrupted sleep at night (must rest when pain is decreased). R: Rest gives patient time to relax and remove self from pain. 7. Teach a method of distraction during acute pain. R: A method of distraction can be used to alleviate pain. 8. Teach non-invasive painrelief measures. (relaxation techniques, music therapy, moment of discussion) R: This are nonpharmacologic methods of reducing pain.
during acute pain. 8. Select and use noninvasive pain-relief measures. (relaxation techniques, music therapy, moment of discussion)
References: Doenges, M., Moorhouse, M. F. & Murr, A. (2006). Nurses pocket guide: Diagnoses, prioritized interventions and rationales. Philadelphia: F.A. Davis Kozier, B., Erb, G., Berman, A. & Snyder, S. (2004). Fundamentals of nursing (7th ed). Philippines: Pearson Prentice Hall Smeltzer, S & Bare, B. (2004). Medical-surgical nursing. N.p.: Lippincott Williams & Wilkins
You might also like
- Basic Rules of The Geneva Conventions and Their Additional ProtocolsDocument32 pagesBasic Rules of The Geneva Conventions and Their Additional ProtocolsInternational Committee of the Red Cross100% (1)
- Inserting A Foley Catheter On A Male Patient: Lecturer: Compiled By: Group 7Document7 pagesInserting A Foley Catheter On A Male Patient: Lecturer: Compiled By: Group 7ratih kusuma dewiNo ratings yet
- Post Operative-Teaching Care PlanDocument9 pagesPost Operative-Teaching Care PlanKit Lara88% (8)
- Dental AnesthesiaDocument20 pagesDental AnesthesiaAnonymous gUjimJKNo ratings yet
- NCP IntraDocument1 pageNCP IntraCharlene Valerie Alviola0% (1)
- Journal Titles and Login CredentialsDocument41 pagesJournal Titles and Login CredentialsAndy F MonroeNo ratings yet
- Alhambra Cigar v. SECDocument3 pagesAlhambra Cigar v. SECAnonymous XvwKtnSrMRNo ratings yet
- FAQs On CARPDocument15 pagesFAQs On CARPMichelleOgatisNo ratings yet
- CSC V BelaganDocument3 pagesCSC V BelaganAnonymous XvwKtnSrMRNo ratings yet
- Case Scenario: Prostate CancerDocument5 pagesCase Scenario: Prostate Cancer24 PAULINO ALDRIN MUJARNo ratings yet
- Nursing Care Plan for Patients with Pancreatic CancerDocument3 pagesNursing Care Plan for Patients with Pancreatic CancerCeliz HilarioNo ratings yet
- NCP CholelithiasisDocument2 pagesNCP Cholelithiasiskmpg11100% (2)
- Complications in Endoscopic Sinus Surgery - Diagnosis, Prevention and Management 2nd EditionDocument241 pagesComplications in Endoscopic Sinus Surgery - Diagnosis, Prevention and Management 2nd EditionRahat tanvirNo ratings yet
- Assessment Nursing Diagnosis Planning Implemantation Rationale EvaluationDocument2 pagesAssessment Nursing Diagnosis Planning Implemantation Rationale EvaluationChloie Marie Rosalejos100% (1)
- Nursing Care Plan On Breast Cancer: Encourage Adequate Rest PeriodsDocument1 pageNursing Care Plan On Breast Cancer: Encourage Adequate Rest PeriodsZen Haven100% (4)
- Case Concerning Oil Platforms (Iran V US)Document9 pagesCase Concerning Oil Platforms (Iran V US)Anonymous XvwKtnSrMRNo ratings yet
- Iglesia Evangelica v. Bishop LazaroDocument3 pagesIglesia Evangelica v. Bishop LazaroAnonymous XvwKtnSrMR100% (1)
- Pathophysiology of Uterine CancerDocument1 pagePathophysiology of Uterine CancerCharlotte Cordero0% (1)
- NCP: Patient With A Pressure UlcerDocument2 pagesNCP: Patient With A Pressure UlcerICa MarlinaNo ratings yet
- Onapal v. CA FPIB v. CADocument5 pagesOnapal v. CA FPIB v. CAAnonymous XvwKtnSrMR0% (1)
- Thyroidectomy Nursing Care PlanDocument2 pagesThyroidectomy Nursing Care PlanRnspeakcom100% (1)
- Nursing Care Plan and Diagnosis For MastectomyDocument4 pagesNursing Care Plan and Diagnosis For MastectomyAngie Mandeoya100% (2)
- Risk for Fluid and Electrolyte ImbalanceDocument3 pagesRisk for Fluid and Electrolyte Imbalancerod navales100% (1)
- NCP - Deficient Fluid VolumeDocument2 pagesNCP - Deficient Fluid VolumerobbychuaNo ratings yet
- Ncp-Modified Redical MastectomyDocument6 pagesNcp-Modified Redical MastectomyMayflor de LunaNo ratings yet
- Nursing Care for Anxiety Related to Upcoming SurgeryDocument1 pageNursing Care for Anxiety Related to Upcoming Surgerynictan 140% (1)
- Care Plan 27Document10 pagesCare Plan 27Oroma TobiasNo ratings yet
- COLON CANCER NCP-impaired nutrITIONDocument3 pagesCOLON CANCER NCP-impaired nutrITIONNicole cuencosNo ratings yet
- Impaired Gas ExchangeDocument2 pagesImpaired Gas ExchangeAura Salve Ildefonso Allas100% (3)
- Super Final NCPDocument16 pagesSuper Final NCPNessaly Jane PrestoNo ratings yet
- NCP - Risk For InfectionDocument2 pagesNCP - Risk For InfectionJet Bautista100% (1)
- NCP Modified Radical MastectomyDocument5 pagesNCP Modified Radical MastectomyIvan Jules P. PALMARESNo ratings yet
- Merrill v. CADocument2 pagesMerrill v. CAAnonymous XvwKtnSrMR50% (2)
- Cosare v. BroadcomDocument4 pagesCosare v. BroadcomAnonymous XvwKtnSrMRNo ratings yet
- Marohombsar v. AlontoDocument2 pagesMarohombsar v. AlontoAnonymous XvwKtnSrMRNo ratings yet
- Memo On Uniform Implementation of DO 174Document3 pagesMemo On Uniform Implementation of DO 174Anonymous XvwKtnSrMR100% (2)
- Nursing Diagnosis and Interventions for LeukemiaDocument6 pagesNursing Diagnosis and Interventions for LeukemiaGeraldine Gallaron - Casipong67% (3)
- NCP For COLON Cancer PatientDocument4 pagesNCP For COLON Cancer PatientCarolina Tardecilla100% (1)
- Magna Financial v. ColarinaDocument3 pagesMagna Financial v. ColarinaAnonymous XvwKtnSrMR100% (1)
- Pathophysiology of Colon Cancer 1Document3 pagesPathophysiology of Colon Cancer 1Katherine Clarisse Carvajal Lavarias100% (1)
- Imbalanced NutritionDocument3 pagesImbalanced NutritionKM100% (6)
- People v. CarantoDocument4 pagesPeople v. CarantoAnonymous XvwKtnSrMR100% (1)
- Ovarian Cancer NCPDocument3 pagesOvarian Cancer NCPEm Emer Emerson0% (5)
- PNB v. PinedaDocument3 pagesPNB v. PinedaAnonymous XvwKtnSrMRNo ratings yet
- Nursing Care Plan for Complicated Grieving and Risk for InjuryDocument6 pagesNursing Care Plan for Complicated Grieving and Risk for InjuryAlex SilvanoNo ratings yet
- NCP PancreatitisDocument2 pagesNCP PancreatitisJeanelle GenerosoNo ratings yet
- Candijay v. CADocument2 pagesCandijay v. CAAnonymous XvwKtnSrMRNo ratings yet
- Coronary Artery Disease Care PlanDocument2 pagesCoronary Artery Disease Care PlanDanelle Harrison, RN100% (2)
- Prostate Cancer NCPDocument1 pageProstate Cancer NCPKathleen Dimacali0% (1)
- Managing Sickle Cell Crisis & Neutropenia in Chemotherapy PatientsDocument3 pagesManaging Sickle Cell Crisis & Neutropenia in Chemotherapy PatientsAnjae GariandoNo ratings yet
- Cancer Nursing Care Plan (NCP) - Risk For InfectionDocument2 pagesCancer Nursing Care Plan (NCP) - Risk For InfectionAngie MandeoyaNo ratings yet
- NCP LymphomaDocument3 pagesNCP LymphomaJohn Emmanuel Tatad TudNo ratings yet
- NCP PainDocument2 pagesNCP PainKarizza Reyes Mamaradlo100% (1)
- Vii. Nursing Care Plan: Secretions in The AirwaysDocument5 pagesVii. Nursing Care Plan: Secretions in The AirwaysJai - Ho100% (2)
- ThyroidectomyDocument2 pagesThyroidectomyYenyen Legas100% (2)
- Nursing Care for FatigueDocument2 pagesNursing Care for FatigueVecky TolentinoNo ratings yet
- Managing Urinary Tract Obstruction Nursing InterventionsDocument8 pagesManaging Urinary Tract Obstruction Nursing Interventionsjyaba0% (1)
- NCP Risk For InfectionDocument6 pagesNCP Risk For InfectionCazze SunioNo ratings yet
- NCP-Esophageal Varices Pleural EffusionDocument6 pagesNCP-Esophageal Varices Pleural Effusiontinatin98933% (3)
- NCP For SchizoDocument6 pagesNCP For SchizoGILIANNE MARIE JIMENEANo ratings yet
- Impaired Skin IntegrityDocument4 pagesImpaired Skin IntegrityVianah Eve EscobidoNo ratings yet
- Nursing Care Plan for Breast CancerDocument2 pagesNursing Care Plan for Breast CancerMaina BarmanNo ratings yet
- Nursing Care Plan for Acute Pain ManagementDocument3 pagesNursing Care Plan for Acute Pain ManagementSheene Lysethea Sioteco AguilosNo ratings yet
- Disturbed Sensory PerceptionDocument3 pagesDisturbed Sensory PerceptionJoenna GaloloNo ratings yet
- Wilm's Tumor Pa Tho PhysiologyDocument1 pageWilm's Tumor Pa Tho Physiologya_yeLNo ratings yet
- TAHBSO ReportDocument4 pagesTAHBSO ReportsachiiMeNo ratings yet
- Nursing Care Plan: Risk For Disuse SyndromeDocument2 pagesNursing Care Plan: Risk For Disuse SyndromeRozsy FakhrurNo ratings yet
- NCPDocument3 pagesNCPChrisTine M. MoralesNo ratings yet
- NCP ErDocument4 pagesNCP ErljarseniornNo ratings yet
- NCP pAlPITATIONSDocument3 pagesNCP pAlPITATIONSHazel PalomaresNo ratings yet
- Nursing Care Plan for Infection and Bleeding PrecautionsDocument6 pagesNursing Care Plan for Infection and Bleeding Precautionshayascent hilarioNo ratings yet
- NCP Stomach CancerDocument2 pagesNCP Stomach CancerJohn Derick BangsoyNo ratings yet
- NCP Activity IntoleranceDocument2 pagesNCP Activity Intolerancea22hous0% (1)
- NCP Proper - Obstructive JaundiceDocument8 pagesNCP Proper - Obstructive JaundiceWyen Cabatbat100% (1)
- Pathophysiology of AMLDocument1 pagePathophysiology of AMLjake251996100% (1)
- Patient Case Study on AppendicitisDocument19 pagesPatient Case Study on Appendicitisfarzaneh yeganehNo ratings yet
- Sas 2 Cabahug, Victoria Mae IDocument4 pagesSas 2 Cabahug, Victoria Mae Ibekbekk cabahugNo ratings yet
- Gnur 405 SuzyDocument6 pagesGnur 405 SuzySeth MensahNo ratings yet
- SCR 270 L & D Care PlanDocument5 pagesSCR 270 L & D Care PlanRenzo MarcosNo ratings yet
- Inter-Country Adoption ReportDocument8 pagesInter-Country Adoption ReportAnonymous XvwKtnSrMRNo ratings yet
- Handbook of Statutory Monetary Benefits 2016 PDFDocument75 pagesHandbook of Statutory Monetary Benefits 2016 PDFAnonymous XvwKtnSrMRNo ratings yet
- DO 18-A Uniform ImplementationDocument3 pagesDO 18-A Uniform ImplementationAl BaljonNo ratings yet
- Simex v. CADocument3 pagesSimex v. CAAnonymous XvwKtnSrMRNo ratings yet
- Comparison of Laws On IncentivesDocument28 pagesComparison of Laws On IncentivesAnonymous XvwKtnSrMRNo ratings yet
- Union Bank vs. CIRDocument6 pagesUnion Bank vs. CIRAnonymous XvwKtnSrMRNo ratings yet
- Salcedo v. ComelecDocument4 pagesSalcedo v. ComelecAnonymous XvwKtnSrMRNo ratings yet
- Salcedo v. ComelecDocument4 pagesSalcedo v. ComelecAnonymous XvwKtnSrMRNo ratings yet
- CBC vs. CADocument2 pagesCBC vs. CAAnonymous XvwKtnSrMRNo ratings yet
- Integrated Realty V CADocument3 pagesIntegrated Realty V CAAnonymous XvwKtnSrMRNo ratings yet
- Hassan v. COMELEC ruling on election failureDocument2 pagesHassan v. COMELEC ruling on election failureAnonymous XvwKtnSrMRNo ratings yet
- Nieva v. Alvarez-EdadDocument2 pagesNieva v. Alvarez-EdadAnonymous XvwKtnSrMRNo ratings yet
- Compiled Digests Letters of CreditDocument9 pagesCompiled Digests Letters of CreditAnonymous XvwKtnSrMRNo ratings yet
- ICC Elements of Crimes PDFDocument50 pagesICC Elements of Crimes PDFKaye de LeonNo ratings yet
- Tax Syllabus (Spit) 2015Document15 pagesTax Syllabus (Spit) 2015Anonymous XvwKtnSrMRNo ratings yet
- TracheotomyDocument4 pagesTracheotomyWilma VeniaNo ratings yet
- Description: Tags: Comp2003awardsDocument17 pagesDescription: Tags: Comp2003awardsanon-595388No ratings yet
- Checklist For Monitoring District Hospital: EmailDocument16 pagesChecklist For Monitoring District Hospital: EmailNational Child Health Resource Centre (NCHRC)No ratings yet
- Oludola Adesina Docx ResumeDocument3 pagesOludola Adesina Docx Resumeapi-355114604No ratings yet
- Medicine in The Ancient WorldDocument20 pagesMedicine in The Ancient Worldpretty JonathanNo ratings yet
- Preface Rhinoplasty: Education Through Multispecialty CollaborationDocument1 pagePreface Rhinoplasty: Education Through Multispecialty CollaborationtuNo ratings yet
- 3d Zygoma ReductionDocument6 pages3d Zygoma ReductionRudolf KiraljNo ratings yet
- Curriculum Vitae Personal DataDocument3 pagesCurriculum Vitae Personal Datarania khedrNo ratings yet
- Clinical Guidelines March 2018 FinalDocument24 pagesClinical Guidelines March 2018 FinalMurad KurdiNo ratings yet
- Surgical Patients UptodateDocument23 pagesSurgical Patients UptodateasmaaNo ratings yet
- POSTOP Impaired Skin Integrity LatestDocument3 pagesPOSTOP Impaired Skin Integrity LatestGel Marie LobatonNo ratings yet
- Carranzas Clinical Periodontology 2nd Southeast Asian Edition PDF Free 10Document219 pagesCarranzas Clinical Periodontology 2nd Southeast Asian Edition PDF Free 10SHUBHAM MALVIYANo ratings yet
- Rehab Guidelines For Reverse Shoulder ArthroplastyDocument7 pagesRehab Guidelines For Reverse Shoulder Arthroplastydeepak100% (1)
- Trabeculectomy Procedure for Lowering Eye PressureDocument42 pagesTrabeculectomy Procedure for Lowering Eye PressureAnita Zhang100% (1)
- C This Is Only A Summary.: Important Questions Answers Why This MattersDocument8 pagesC This Is Only A Summary.: Important Questions Answers Why This MattersChris DuffnerNo ratings yet
- Critical View of SafetyDocument4 pagesCritical View of SafetyIntan Eklesiana NapitupuluNo ratings yet
- Juan Sumulong High School: English For Academic PurposesDocument59 pagesJuan Sumulong High School: English For Academic Purposespeter vanderNo ratings yet
- NRLS 0236 Wristbands SPN 2005 11 22 v1Document6 pagesNRLS 0236 Wristbands SPN 2005 11 22 v1irene damanikNo ratings yet
- Pain Free ProgramDocument70 pagesPain Free ProgramNurul SyuhaidahNo ratings yet
- Laparoscopic Entry After Previous Surgery: Tips and TechniquesDocument3 pagesLaparoscopic Entry After Previous Surgery: Tips and TechniquesMohmd AboelkheirNo ratings yet
- Distraction Osteogenesis For Ridge Augmentation PR PDFDocument11 pagesDistraction Osteogenesis For Ridge Augmentation PR PDFMuaiyed Buzayan AkremyNo ratings yet
- Delayed Diagnosis of Ischemia After Popliteal Artery Injury During Total Knee ArthroplastyDocument4 pagesDelayed Diagnosis of Ischemia After Popliteal Artery Injury During Total Knee ArthroplastyHerald Scholarly Open AccessNo ratings yet
- Civil Service Form GuideDocument3 pagesCivil Service Form GuideStephanie PayumoNo ratings yet
- Funda Rle PrelimsDocument13 pagesFunda Rle PrelimsIvan MaximusNo ratings yet
- Millenium Gold Medal Award 2021Document1 pageMillenium Gold Medal Award 2021Shiwali SinghNo ratings yet
- Sodium Hypochlorite Is More Effective Than Chlorhexidine For Eradication of Bacterial Biofilm of Staphylococci and PseudomonasDocument7 pagesSodium Hypochlorite Is More Effective Than Chlorhexidine For Eradication of Bacterial Biofilm of Staphylococci and Pseudomonashalil dalçinNo ratings yet