You might also like
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- Systemic Lupus Erythematosus: Basic, Applied and Clinical AspectsFrom EverandSystemic Lupus Erythematosus: Basic, Applied and Clinical AspectsGeorge C. TsokosNo ratings yet
- Patho4-6 - Liver (Dr. Dy)Document13 pagesPatho4-6 - Liver (Dr. Dy)miguel cuevas100% (1)
- Patho A 1. 5 Hemodynamic Disorders (Bongat, 2015)Document12 pagesPatho A 1. 5 Hemodynamic Disorders (Bongat, 2015)Grant GarcesNo ratings yet
- Pathology Cell InjuryDocument57 pagesPathology Cell InjuryMajd MustafaNo ratings yet
- Robbin's SummariesDocument98 pagesRobbin's SummariesnopedontsuemepleaseNo ratings yet
- Endocrine PathologyDocument13 pagesEndocrine Pathologysarguss14100% (1)
- GI PathologyDocument22 pagesGI Pathologyzeroun24100% (5)
- GASTROINSTINAL TRACT Robbins 8th EditionDocument4 pagesGASTROINSTINAL TRACT Robbins 8th EditionLim EricNo ratings yet
- Renal Pathology Lectures - PPT SeriesDocument267 pagesRenal Pathology Lectures - PPT SeriesMarc Imhotep Cray, M.D.100% (12)
- Endocrine Gland Hormone(s) Secreted Stimulus Effect of Hormone Inhibition PathologyDocument3 pagesEndocrine Gland Hormone(s) Secreted Stimulus Effect of Hormone Inhibition PathologySamuelNo ratings yet
- Endocrine System - Part 1 (Robbins)Document28 pagesEndocrine System - Part 1 (Robbins)sarguss14100% (2)
- Inflammation and Repair OverviewDocument10 pagesInflammation and Repair OverviewMiguel Cuevas DolotNo ratings yet
- Endocrine Pathology p17-32Document16 pagesEndocrine Pathology p17-32zeroun24No ratings yet
- General Pathology Bimonthly Exam Compilation Updated 2Document197 pagesGeneral Pathology Bimonthly Exam Compilation Updated 2Cherry Rahima100% (1)
- Cell Injury & AdaptationDocument22 pagesCell Injury & AdaptationUmam LoyalNo ratings yet
- Pathology of Liver, Biliary, and PancreasDocument52 pagesPathology of Liver, Biliary, and PancreasHassan.shehri100% (11)
- Robbins Ch. 20 The Kidney Review QuestionsDocument10 pagesRobbins Ch. 20 The Kidney Review QuestionsPA2014100% (4)
- Robbins Ch. 26 Bones Joints and Soft-Tissue Tumors Review QuestionsDocument7 pagesRobbins Ch. 26 Bones Joints and Soft-Tissue Tumors Review QuestionsPA2014100% (1)
- Top 100 Pathology Secrets List W/ NotesDocument6 pagesTop 100 Pathology Secrets List W/ NotesPA2014100% (4)
- Chapter 11 Blood Vessels 8th Ed NotesDocument7 pagesChapter 11 Blood Vessels 8th Ed NotesKyle Christopher SiaNo ratings yet
- Cellular Injury, Adaptation and Cell DeathDocument8 pagesCellular Injury, Adaptation and Cell DeathJessica Febrina Wuisan100% (1)
- Hemodynamic Disorders, Thromboembolic Disease, and ShockDocument87 pagesHemodynamic Disorders, Thromboembolic Disease, and Shockgifty100% (1)
- Genetic and Pediatric Diseases Chapter SummaryDocument16 pagesGenetic and Pediatric Diseases Chapter SummaryJustine HungNo ratings yet
- Chapter 5 (Questions 2008-2009 Compiled)Document28 pagesChapter 5 (Questions 2008-2009 Compiled)vetpathforumNo ratings yet
- Chapter 10 - Diseases of Infancy and ChildhoodDocument17 pagesChapter 10 - Diseases of Infancy and ChildhoodAgnieszka WisniewskaNo ratings yet
- Endocrine PathologyDocument31 pagesEndocrine PathologyAnonymous 49jFPGI5KN100% (1)
- Cardiac Physiology & Pathology TopicsDocument3 pagesCardiac Physiology & Pathology TopicsByeongsu Park100% (1)
- Patho - Inflammation SummaryDocument28 pagesPatho - Inflammation SummaryTep Gonzales71% (7)
- Robbins and Cotran's Pathologic Basis of Disease Chapter 1Document14 pagesRobbins and Cotran's Pathologic Basis of Disease Chapter 1Mon Dominguez100% (2)
- Acute Inflammation - Robbins Basic Pathology - Inflammation & RepairDocument24 pagesAcute Inflammation - Robbins Basic Pathology - Inflammation & RepairLuis Adrian De Jesús100% (9)
- Robbins Questions Chp1-10Document28 pagesRobbins Questions Chp1-10verbatimmt100% (1)
- Ch.1 Baby Robbins OutlineDocument11 pagesCh.1 Baby Robbins OutlinePA2014100% (3)
- Robbins Basic Pathology 9th Edition QBankDocument4 pagesRobbins Basic Pathology 9th Edition QBankVarshini Tamil SelvanNo ratings yet
- SURGPATH - 2.1 The Gastrointestinal Tract (Robbins) - TableDocument8 pagesSURGPATH - 2.1 The Gastrointestinal Tract (Robbins) - TableAngela Caguitla100% (1)
- P.G. Curriculum M.D. Pathology Index: 1. GoalDocument18 pagesP.G. Curriculum M.D. Pathology Index: 1. GoalAvwan DududNo ratings yet
- Liver - RobbinsDocument25 pagesLiver - Robbinssarguss14100% (2)
- WBC Pathology: Lecturer: Associate Professor T. A. GrekovaDocument49 pagesWBC Pathology: Lecturer: Associate Professor T. A. GrekovaFaheem MusthafaNo ratings yet
- DB13 - Pathophysiology of AtherosclerosisDocument2 pagesDB13 - Pathophysiology of Atherosclerosisi_vhie03No ratings yet
- Renal Vascular Disease GuideDocument46 pagesRenal Vascular Disease GuideCoy NuñezNo ratings yet
- Pancreatic Hormones and Antidiabetic AgentsDocument3 pagesPancreatic Hormones and Antidiabetic AgentsChristian DeeNo ratings yet
- CardiacArrhythmiasPathophysiology PDFDocument1 pageCardiacArrhythmiasPathophysiology PDFNeelam Raj ThakurNo ratings yet
- Hyperthyroidism: DR Rajeshwar ReddyDocument59 pagesHyperthyroidism: DR Rajeshwar ReddyRajeshwarreddy RamaswamyNo ratings yet
- Introduction to Pathology: Study of Disease at the Cellular LevelDocument44 pagesIntroduction to Pathology: Study of Disease at the Cellular Level53-Deepankar SutradharNo ratings yet
- Chapter 7 Neoplasia 1 2 Robbins and Cotran Pathologic Basis of Disease PDFDocument9 pagesChapter 7 Neoplasia 1 2 Robbins and Cotran Pathologic Basis of Disease PDFChethranNo ratings yet
- Thyroid Gland DisordersDocument64 pagesThyroid Gland DisordersFaisal RavifNo ratings yet
- Pathology GlomerulonephritisDocument4 pagesPathology GlomerulonephritisGerardLum100% (2)
- Anca VasculitisDocument12 pagesAnca Vasculitisatul_desai_3100% (2)
- Robbins Pathology Chapter 13 - White Blood CellsDocument7 pagesRobbins Pathology Chapter 13 - White Blood Cellsscorpiosphinx7980% (5)
- EBM - 5. Adrenal DisordersDocument101 pagesEBM - 5. Adrenal DisordersBRI KUNo ratings yet
- Robbins Pathology Chapter 14 - RBCsDocument7 pagesRobbins Pathology Chapter 14 - RBCsscorpiosphinx79100% (10)
- Gastrointestinal PathologyDocument14 pagesGastrointestinal PathologyRahul ShuklaNo ratings yet
- Cell Injury and Cell DeathDocument35 pagesCell Injury and Cell DeathMarc Imhotep Cray, M.D.No ratings yet
- Robbin's Chapter 20 Kidney PathologyDocument4 pagesRobbin's Chapter 20 Kidney Pathologynbaumgartner0100% (1)
- Git PathologyDocument113 pagesGit PathologyanggitaNo ratings yet
- Causes, Types and Morphology of Cell Injury and DeathDocument18 pagesCauses, Types and Morphology of Cell Injury and DeathYoja GarzonNo ratings yet
- Liver PathologyDocument21 pagesLiver Pathologyzeroun24100% (6)
- Skin Summary ChartDocument7 pagesSkin Summary ChartMarco HernandezNo ratings yet
- Conn Syndrome, (Hyper-Aldosteronism) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandConn Syndrome, (Hyper-Aldosteronism) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- DIT Study GuideDocument10 pagesDIT Study Guideaagarwalmd0% (1)
- Robbins Pathology Chapter 13 - White Blood CellsDocument7 pagesRobbins Pathology Chapter 13 - White Blood Cellsscorpiosphinx7980% (5)
- Robbins Pathology Chapter 17 Liver and Biliary TractDocument2 pagesRobbins Pathology Chapter 17 Liver and Biliary Tractscorpiosphinx79No ratings yet
- Robbins Pathology Chapter 14 - RBCsDocument7 pagesRobbins Pathology Chapter 14 - RBCsscorpiosphinx79100% (10)
- READING PRACTICE TEST 3Document9 pagesREADING PRACTICE TEST 3Cao Son Dang Vu0% (1)
- Application of Fascial Manipulation Technique in Chronic Shoulder PainDocument9 pagesApplication of Fascial Manipulation Technique in Chronic Shoulder PainIsabelGuijarroMartinez100% (1)
- I. Objectives A. Content Standards: Monday Tuesday Wednesday Thursday FridayDocument8 pagesI. Objectives A. Content Standards: Monday Tuesday Wednesday Thursday FridayMaribel NayadNo ratings yet
- Yoga Class 12Document13 pagesYoga Class 12Vandan KNo ratings yet
- Exploring Creation With Advanced Biology 2 Edition - Errata: Textbook - 1 and 2 PrintingsDocument2 pagesExploring Creation With Advanced Biology 2 Edition - Errata: Textbook - 1 and 2 PrintingsJacquie ScholeNo ratings yet
- Hormone Practice Test: StudentDocument17 pagesHormone Practice Test: StudentKayne SuratosNo ratings yet
- Components of Blood - Red Blood Cells, White Blood Cells, and PlateletsDocument20 pagesComponents of Blood - Red Blood Cells, White Blood Cells, and PlateletsVishal SharmaNo ratings yet
- CNS Development and OrganizationDocument6 pagesCNS Development and OrganizationKhamron BridgewaterNo ratings yet
- How Do We Take Care of Our Endocrine SystemDocument7 pagesHow Do We Take Care of Our Endocrine SystemAndrei CunananNo ratings yet
- Hemato OnologyDocument60 pagesHemato OnologyGousayAlkhazmariNo ratings yet
- Surface Anatomy: de La Salle-Lipa College of LawDocument79 pagesSurface Anatomy: de La Salle-Lipa College of LawFatzie MendozaNo ratings yet
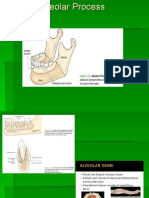
- Alveolar BoneDocument24 pagesAlveolar BoneHanna SouthwellNo ratings yet
- Anatomicallandmarksofdenturebearingareaof 130812025925 Phpapp02Document48 pagesAnatomicallandmarksofdenturebearingareaof 130812025925 Phpapp02AnimeAngelNo ratings yet
- Hema - Cytochemistry With TablesDocument4 pagesHema - Cytochemistry With TablesAce TardoNo ratings yet
- Hemostasis and Platelet FunctionDocument17 pagesHemostasis and Platelet FunctionUzama Binu AliNo ratings yet
- Digestive System Part 2 Large Intestine Water and Mineral AbsorptionDocument16 pagesDigestive System Part 2 Large Intestine Water and Mineral AbsorptionFhayee Sulaik HaronNo ratings yet
- Reproductive Health Guide Matches Key PartsDocument2 pagesReproductive Health Guide Matches Key Partsalan patinoNo ratings yet
- Blok 10 03.11.2017Document174 pagesBlok 10 03.11.2017VaniaNo ratings yet
- Hydatidosis: A Mystery Box at Various SitesDocument7 pagesHydatidosis: A Mystery Box at Various SitesIJAR JOURNALNo ratings yet
- Chapter 7 CELL STRUCTURE AND FUNCTION PDFDocument16 pagesChapter 7 CELL STRUCTURE AND FUNCTION PDFAngelene PelayoNo ratings yet
- Bradycardia & TachycardiaDocument14 pagesBradycardia & TachycardiaHendri SaputraNo ratings yet
- PAS Stain Procedure and Fixatives in HistochemistryDocument18 pagesPAS Stain Procedure and Fixatives in HistochemistryParveen AkhtarNo ratings yet
- Uddin Et Al., 2022Document4 pagesUddin Et Al., 2022James BondNo ratings yet
- Materi Digestive SystemDocument13 pagesMateri Digestive Systembetta putriNo ratings yet
- Mythic18 Alarms ExplanationDocument4 pagesMythic18 Alarms ExplanationNelsonNo ratings yet
- PhysiologyDocument5 pagesPhysiologyCpopNo ratings yet
- Understanding Hypothyroidism: Causes, Symptoms and TreatmentDocument14 pagesUnderstanding Hypothyroidism: Causes, Symptoms and TreatmentMari IllustriousNo ratings yet
- Primary Abdominal Ectopic Pregnancy: A Case ReportDocument4 pagesPrimary Abdominal Ectopic Pregnancy: A Case ReportYared TJNo ratings yet
- Science Quest 8 AC 3E c04 PDFDocument94 pagesScience Quest 8 AC 3E c04 PDFmaxx100% (1)
- Chapter No. 3 4 Gerontological NursingDocument110 pagesChapter No. 3 4 Gerontological NursingHerman ZoletaNo ratings yet