You might also like
- EKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!From EverandEKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!No ratings yet
- The 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsFrom EverandThe 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsNo ratings yet
- Cardiac Dysrhythmia Chart Med Surg NUR4 PDFDocument3 pagesCardiac Dysrhythmia Chart Med Surg NUR4 PDFlml100% (1)
- ECG StripsDocument5 pagesECG Stripssurviving nursing school100% (1)
- EKG | ECG: An Ultimate Step-By-Step Guide to 12-Lead EKG | ECG Interpretation, Rhythms & Arrhythmias Including Basic Cardiac DysrhythmiasFrom EverandEKG | ECG: An Ultimate Step-By-Step Guide to 12-Lead EKG | ECG Interpretation, Rhythms & Arrhythmias Including Basic Cardiac DysrhythmiasRating: 3 out of 5 stars3/5 (5)
- EKG | ECG Interpretation. Everything You Need to Know about 12-Lead ECG/EKG InterpretationFrom EverandEKG | ECG Interpretation. Everything You Need to Know about 12-Lead ECG/EKG InterpretationRating: 3 out of 5 stars3/5 (1)
- Cardiac DysrhythmiasDocument3 pagesCardiac DysrhythmiasKatherine Santiago92% (62)
- Basic Arrhythmia RulesDocument3 pagesBasic Arrhythmia Rulesgreenflames0997% (30)
- EKG ExamplesDocument9 pagesEKG ExamplesMayer Rosenberg99% (235)
- Dysrhythmias ChartDocument6 pagesDysrhythmias Chartjkrix100% (1)
- ECG Interpretation Cheat SheetDocument1 pageECG Interpretation Cheat Sheethirsi20051879% (24)
- Cardiac Study GuideDocument11 pagesCardiac Study Guidejenwiley318096% (73)
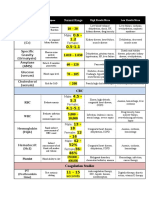
- Lab ValuesDocument3 pagesLab Valuessurviving nursing school100% (1)
- ArrhythmiaDocument2 pagesArrhythmiaChris Pritchard93% (30)
- Acid-Base WorksheetDocument2 pagesAcid-Base WorksheetMayer Rosenberg100% (18)
- Cardiac DrugsDocument10 pagesCardiac DrugsNursePoor98% (47)
- A Simplified ECG GuideDocument4 pagesA Simplified ECG Guidejalan_z96% (27)
- EKG Cheat SheetDocument9 pagesEKG Cheat SheetAlert Twitter100% (5)
- ABG InterpretationDocument1 pageABG Interpretationnulall100% (18)
- ACLS EKG Rhythms and InterpretationDocument10 pagesACLS EKG Rhythms and Interpretationdonheyzz_02No ratings yet
- Cardiac Meds ChartDocument1 pageCardiac Meds ChartCharlotte Louise75% (4)
- Cardiac Med ChartsDocument6 pagesCardiac Med ChartsNursingSchoolNotes100% (15)
- EKG Flash CardsDocument5 pagesEKG Flash CardsRyann Sampino FreitasNo ratings yet
- Spotlight On Cardiac DrugsDocument2 pagesSpotlight On Cardiac Drugspauerish100% (2)
- Reading A EKGDocument10 pagesReading A EKGMayer Rosenberg100% (15)
- May/No P: Inverted/B/ A Qrs P (Befor e QRS) - 0.12Document3 pagesMay/No P: Inverted/B/ A Qrs P (Befor e QRS) - 0.12is_aradanas0% (1)
- Ekg Guidelines PDFDocument7 pagesEkg Guidelines PDFd.ramadhan100% (1)
- Ecg Cheat Sheet 35Document2 pagesEcg Cheat Sheet 35jessjaylee80% (5)
- ECG ReadingDocument11 pagesECG ReadingSuresh Shrestha100% (1)
- Basic EKG ECG Rhythms CheatsheetDocument1 pageBasic EKG ECG Rhythms CheatsheetAhmad83% (6)
- ABG Made EasyDocument10 pagesABG Made EasyMayer Rosenberg100% (38)
- Dysrhythmia Recognition Pocket Reference Card PDFDocument14 pagesDysrhythmia Recognition Pocket Reference Card PDFjenn1722100% (2)
- Cardiac DrugsDocument5 pagesCardiac Drugseric100% (17)
- Pakya ECG BasicsDocument5 pagesPakya ECG BasicsFrederick CokroNo ratings yet
- EKG Flash Cards PDFDocument9 pagesEKG Flash Cards PDFdiani arisandhi100% (1)
- Common Cardiac MedicationsDocument1 pageCommon Cardiac MedicationsPaige HardekopfNo ratings yet
- Schaum's Outline of Critical Care Nursing: 250 Review QuestionsFrom EverandSchaum's Outline of Critical Care Nursing: 250 Review QuestionsRating: 5 out of 5 stars5/5 (1)
- FAMILY NURSE PRACTITIONER: Passbooks Study GuideFrom EverandFAMILY NURSE PRACTITIONER: Passbooks Study GuideNo ratings yet
- ECG & EKG Interpretation: How to interpret ECG & EKG, including rhythms, arrhythmias, and more!From EverandECG & EKG Interpretation: How to interpret ECG & EKG, including rhythms, arrhythmias, and more!No ratings yet
- Advance Cardiac Life Support: Short, Sweet and to the PointFrom EverandAdvance Cardiac Life Support: Short, Sweet and to the PointRating: 3 out of 5 stars3/5 (2)
- Cardiac Tamponade, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCardiac Tamponade, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Nurse Practitioner Board ReviewFrom EverandNurse Practitioner Board ReviewRating: 5 out of 5 stars5/5 (1)
- Adult CCRN Exam Flashcards, Second Edition: Up-to-Date Review and PracticeFrom EverandAdult CCRN Exam Flashcards, Second Edition: Up-to-Date Review and PracticeRating: 5 out of 5 stars5/5 (1)
- Family Nurse Practitioner Certification Prep Plus: Proven Strategies + Content Review + Online PracticeFrom EverandFamily Nurse Practitioner Certification Prep Plus: Proven Strategies + Content Review + Online PracticeRating: 5 out of 5 stars5/5 (2)
- This Study Resource Was Shared Via: Sinus BradycardiaDocument3 pagesThis Study Resource Was Shared Via: Sinus BradycardiaPascal St Peter NwaorguNo ratings yet
- KRIZELDocument13 pagesKRIZELKrizel Adina TanNo ratings yet
- Ecg 2Document10 pagesEcg 2AANo ratings yet
- Cardiology-5 DysrhythmiaDocument16 pagesCardiology-5 DysrhythmiaMahmoud RamadanNo ratings yet
- WSBB Guide For Beginners - Bench-CompressedDocument15 pagesWSBB Guide For Beginners - Bench-CompressedKatya KNo ratings yet
- Hijama Cupping PDFDocument16 pagesHijama Cupping PDFMuhammad Khalid JavedNo ratings yet
- Review of Related LiteratureDocument27 pagesReview of Related Literatureme langNo ratings yet
- Charter of Patient's RightsDocument41 pagesCharter of Patient's RightsHarsh Sharma100% (1)
- Individual Development Plan FormDocument2 pagesIndividual Development Plan FormLielet MatutinoNo ratings yet
- Timms 1980Document8 pagesTimms 1980Zahid ManzoorNo ratings yet
- The Mediating Role of Emotional Intelligence in The Employees PerformanceDocument11 pagesThe Mediating Role of Emotional Intelligence in The Employees PerformanceMårkö ÅlexövåNo ratings yet
- 9.2 Group A 9.4 Group A: Exercise 1 Exercise 1Document1 page9.2 Group A 9.4 Group A: Exercise 1 Exercise 1Carolina Fernández DoradoNo ratings yet
- Pattern and Associated Factors of Exam Anxiety Among Students of Private Medical College PakistanDocument3 pagesPattern and Associated Factors of Exam Anxiety Among Students of Private Medical College PakistanBahadur AliNo ratings yet
- 0121 Letter Directing Employee To Undertake Fitness Work AssessmentDocument2 pages0121 Letter Directing Employee To Undertake Fitness Work AssessmentRobin james PardilloNo ratings yet
- Ncbts Domain 5Document2 pagesNcbts Domain 5Maureen Mae Estanol100% (1)
- MIDTERM Gender and Society GUIDESDocument8 pagesMIDTERM Gender and Society GUIDESJasher JoseNo ratings yet
- Unit 8 Iso 22000:2005 - An Overview: StructureDocument20 pagesUnit 8 Iso 22000:2005 - An Overview: Structuregsakthivel2008No ratings yet
- Entry 3 Reading Sample Paper 1 CA v3 Dec17Document10 pagesEntry 3 Reading Sample Paper 1 CA v3 Dec17lilalilak0% (1)
- Research Article: ISSN: 0975-833XDocument5 pagesResearch Article: ISSN: 0975-833XSoumya prakash HotaNo ratings yet
- Five Year Plans of India..Document27 pagesFive Year Plans of India..Nalin08100% (11)
- SIC - 01252 Sickness NotificationDocument3 pagesSIC - 01252 Sickness NotificationJeannylyn BurgosNo ratings yet
- Amercor 8760 BM ENGDocument12 pagesAmercor 8760 BM ENGchoppersureNo ratings yet
- Project Report On Hospital - 100 BedsDocument3 pagesProject Report On Hospital - 100 BedsEIRI Board of Consultants and Publishers100% (1)
- Laboratory Activity 11 - Respiratory System1Document4 pagesLaboratory Activity 11 - Respiratory System1Kiane Dominique GarotNo ratings yet
- Classroom AbusesDocument6 pagesClassroom AbusesJulius de la CruzNo ratings yet
- BP Open Sampling & Additivisation Procedure 1 - 0Document51 pagesBP Open Sampling & Additivisation Procedure 1 - 0ParaZzzitNo ratings yet
- 5 Basic Survival TechniquesDocument5 pages5 Basic Survival TechniquesAngelika IngosanNo ratings yet
- Group 2 - Final Iii PDFDocument79 pagesGroup 2 - Final Iii PDFMaureen FloresNo ratings yet
- Disorders of The Nervous System2Document20 pagesDisorders of The Nervous System2Ian Rizavi Villamor AntopinaNo ratings yet
- PAS Preschool Anxiety Scale Blank FormDocument3 pagesPAS Preschool Anxiety Scale Blank FormKhansa ChaudaryNo ratings yet
- ResearchDocument14 pagesResearchShannel SanzNo ratings yet
- Classroom Observation 4th Quarter LessonDocument4 pagesClassroom Observation 4th Quarter LessonKen AlonzoNo ratings yet
- T File To PrintDocument6 pagesT File To Printanna.mary.arueta.gintoro031202No ratings yet
- Herbal Drugs For Thyroid - PDF: International Journal of Pharmacy and Biological Sciences May 2016Document10 pagesHerbal Drugs For Thyroid - PDF: International Journal of Pharmacy and Biological Sciences May 2016Sanju TkNo ratings yet