You might also like
- Postnatal Assessment ProcedureDocument4 pagesPostnatal Assessment ProcedureApex College of Nursing100% (2)
- Postnatal AssessmentDocument11 pagesPostnatal AssessmentNeelofur Ibran Ali91% (46)
- PRO Post Natal AssessmentDocument9 pagesPRO Post Natal AssessmentMali KanuNo ratings yet
- Government College of Nursing:, Jodhpur (Raj.)Document7 pagesGovernment College of Nursing:, Jodhpur (Raj.)priyankaNo ratings yet
- Gynecological ProceduresDocument17 pagesGynecological Proceduresjeelani saima100% (5)
- Demonstration POSTNATAL EXAMINATION Easy WayDocument9 pagesDemonstration POSTNATAL EXAMINATION Easy Wayjyoti singhNo ratings yet
- Intranatal Assessment Kempegowda College of Nursing, V.V.Puram, B'Lore-04Document8 pagesIntranatal Assessment Kempegowda College of Nursing, V.V.Puram, B'Lore-04Vijith.V.kumar100% (1)
- Antenatal Assessment FormatDocument9 pagesAntenatal Assessment FormatVijith.V.kumar93% (14)
- Antenatal ExaminationDocument5 pagesAntenatal ExaminationAnuradha MauryaNo ratings yet
- Unit 3 - Antenatal AssessmentDocument9 pagesUnit 3 - Antenatal AssessmentN. Siva100% (4)
- Health Talk On Antenatl ExerciseDocument12 pagesHealth Talk On Antenatl ExerciseRavina Patel75% (12)
- Procedure Antenatal Assessment - 1Document6 pagesProcedure Antenatal Assessment - 1Kinjal Vasava92% (12)
- Intranatal Assessment FormatDocument10 pagesIntranatal Assessment FormatAnnapurna Dangeti100% (1)
- Antenatal ExaminationDocument18 pagesAntenatal ExaminationAnonymous ExR0zw100% (2)
- Antenatal Assessment FormatDocument9 pagesAntenatal Assessment FormatPalaniswami Palaniswami67% (3)
- Postnatal Assessment FormatDocument16 pagesPostnatal Assessment FormatValarmathi92% (13)
- Antenatal ExercisesDocument45 pagesAntenatal ExercisesLahunWanniang100% (2)
- Antenatal-Exercises Health EducationDocument13 pagesAntenatal-Exercises Health EducationBlessy Madhuri100% (2)
- Postnatel Examination (Procedure)Document20 pagesPostnatel Examination (Procedure)Raja100% (3)
- Procedure ON: Copper-T InsertionDocument5 pagesProcedure ON: Copper-T Insertionpriyanka100% (2)
- Lesson Plan On Post Natal ExercisesDocument11 pagesLesson Plan On Post Natal ExercisesRaja67% (6)
- Instruments FileDocument27 pagesInstruments Filepriyanka100% (2)
- Health Edu - On Postnatal ExerciseDocument16 pagesHealth Edu - On Postnatal Exercisepriyanka88% (8)
- Antenatal Care & Management NewDocument23 pagesAntenatal Care & Management NewPabhat Kumar100% (4)
- Practical - 7 Antenatal ClinicDocument17 pagesPractical - 7 Antenatal ClinicSujatha J JayabalNo ratings yet
- Lesson Plan On Post Natal ExercisesDocument11 pagesLesson Plan On Post Natal Exercisesvarshasharma0593% (15)
- Antenatal Diet PlanDocument7 pagesAntenatal Diet PlanSunija Selvam100% (3)
- ANTENATAL Case Study FormatDocument4 pagesANTENATAL Case Study FormatDelphy Varghese100% (8)
- Procedure Manual For Obstetrics and Gynecological Nursing: Government College of Nursing Somajiguda, Hyderabad, T.SDocument119 pagesProcedure Manual For Obstetrics and Gynecological Nursing: Government College of Nursing Somajiguda, Hyderabad, T.SBlessy Madhuri100% (5)
- Government College of Nursing Jodhpur (Raj.) : Procedure On-Amniocentesis Subject-Obstetrics & Gynaecology Specialty-IDocument7 pagesGovernment College of Nursing Jodhpur (Raj.) : Procedure On-Amniocentesis Subject-Obstetrics & Gynaecology Specialty-Ipriyanka100% (1)
- Newborn Assessment OBGDocument6 pagesNewborn Assessment OBGAnish VeettiyankalNo ratings yet
- Postnatal CareDocument26 pagesPostnatal CareShivani Shah100% (1)
- Effect of Drug During Pregnancy, Labour and PuerperiumDocument10 pagesEffect of Drug During Pregnancy, Labour and PuerperiumSabeethu Girija63% (16)
- Era University / Era College of Nursing: Lesson Plan On-InfertilityDocument11 pagesEra University / Era College of Nursing: Lesson Plan On-InfertilityShreya Sinha100% (3)
- Placental ExaminationDocument12 pagesPlacental ExaminationNidhi Sharma100% (7)
- Unit-2 Antenatal AssessmentDocument16 pagesUnit-2 Antenatal AssessmentAnil Patel100% (5)
- Evidence Based Practices in Obstetrical and Gynaecological NursingDocument40 pagesEvidence Based Practices in Obstetrical and Gynaecological Nursingpratibhakamath97% (30)
- Lesson Pla1Document9 pagesLesson Pla1annu panchal100% (1)
- Demonstration On EpisiotomyDocument11 pagesDemonstration On EpisiotomyBabita DhruwNo ratings yet
- EpisiotomyDocument6 pagesEpisiotomyNishaThakuri100% (1)
- Antenatal AssessmentDocument16 pagesAntenatal AssessmentDevuchandana RNo ratings yet
- Lesson Plan On Manual Removal of Placenta: Submitted ToDocument10 pagesLesson Plan On Manual Removal of Placenta: Submitted Tocharanjit kaurNo ratings yet
- Antenatal Abdominal ExaminationDocument5 pagesAntenatal Abdominal Examinationjyoti kundu100% (2)
- Clinical Presentation On ObgDocument20 pagesClinical Presentation On ObgValarmathiNo ratings yet
- Cs Breast EngorgementDocument14 pagesCs Breast Engorgementamit85% (13)
- Forceps DeliveryDocument22 pagesForceps DeliveryN. Siva100% (1)
- Health Talk Om Antenatal ExerciseDocument10 pagesHealth Talk Om Antenatal ExercisePiyush Dutta100% (7)
- Checklist For Antenatal AssessmentDocument4 pagesChecklist For Antenatal Assessmentbaby92% (12)
- Lesson Plan On Uterine Abnormality and Displacement: B.SC Nursing StudentsDocument20 pagesLesson Plan On Uterine Abnormality and Displacement: B.SC Nursing StudentsKinjal VasavaNo ratings yet
- Menstrual Irregularities FinalDocument24 pagesMenstrual Irregularities Finalksmad_268741100% (2)
- Antenatal ExerciseDocument18 pagesAntenatal ExerciseBindu Philip100% (2)
- ANTENATAL ASSESSMENT Form 4Document4 pagesANTENATAL ASSESSMENT Form 4Kaku Manisha100% (4)
- 3rd Stage of LabourDocument22 pages3rd Stage of Labourvarshasharma05100% (6)
- Management of Woman During First Stage of Labour Management of Woman During First Stage of LabourDocument21 pagesManagement of Woman During First Stage of Labour Management of Woman During First Stage of LabourKinjal Vasava67% (3)
- Fourth Stage of Labour SubmissionDocument21 pagesFourth Stage of Labour SubmissionSavita HanamsagarNo ratings yet
- Obgyn SL1Document39 pagesObgyn SL1mustafe omarNo ratings yet
- Management of The First Stage of Labour LectureDocument48 pagesManagement of The First Stage of Labour LectureJSeashark100% (3)
- Guidelines Postpartum AssessmentDocument2 pagesGuidelines Postpartum Assessmentgrad_nurse_2015100% (1)
- Antenatal Examination According To WHODocument6 pagesAntenatal Examination According To WHOManisha ThakurNo ratings yet
- Nursing Care of Family During Labor and BirthhhDocument6 pagesNursing Care of Family During Labor and BirthhhAudreySalvadorNo ratings yet
- Breast CancerDocument15 pagesBreast CancerVijith.V.kumar100% (2)
- Expanded RoleDocument19 pagesExpanded RoleVijith.V.kumar100% (2)
- Forceps DeliveryDocument32 pagesForceps DeliveryVijith.V.kumar50% (2)
- Occipito Posterior PositionDocument52 pagesOccipito Posterior PositionVijith.V.kumar100% (3)
- Advanced Neonatal Procedures2Document14 pagesAdvanced Neonatal Procedures2Vijith.V.kumar100% (8)
- Staff Orientation, Training and DevelopmentDocument57 pagesStaff Orientation, Training and DevelopmentVijith.V.kumarNo ratings yet
- Records and ReportsDocument6 pagesRecords and ReportsVijith.V.kumar100% (5)
- Breech PresentationDocument53 pagesBreech PresentationVijith.V.kumar100% (6)
- Premature BabyDocument41 pagesPremature BabyVijith.V.kumar100% (9)
- CPDDocument45 pagesCPDVijith.V.kumar100% (1)
- Antenatal PreparationDocument47 pagesAntenatal PreparationVijith.V.kumarNo ratings yet
- Obstetric EmergenciesDocument44 pagesObstetric EmergenciesVijith.V.kumarNo ratings yet
- Uterine Anomaly, Fibroid Uterus, Ovarian Tumor, Uterine ProlapseDocument30 pagesUterine Anomaly, Fibroid Uterus, Ovarian Tumor, Uterine ProlapseVijith.V.kumar80% (5)
- Gynecological DisordersDocument26 pagesGynecological DisordersVijith.V.kumarNo ratings yet
- Destructive Operation and Caesarian SectionDocument53 pagesDestructive Operation and Caesarian SectionVijith.V.kumar0% (1)
- High Risk NewbornDocument76 pagesHigh Risk NewbornVijith.V.kumar91% (22)
- Neonatal NursingDocument2 pagesNeonatal NursingVijith.V.kumarNo ratings yet
- Diet During PregnancyDocument14 pagesDiet During PregnancyVijith.V.kumarNo ratings yet
- Analgesia and Anesthesia in ObstetricsDocument8 pagesAnalgesia and Anesthesia in ObstetricsVijith.V.kumar100% (3)
- Kempegowda College of Nursing: Subject: Obstetric and Gynaecological NursingDocument2 pagesKempegowda College of Nursing: Subject: Obstetric and Gynaecological NursingVijith.V.kumarNo ratings yet
- Phisiological Changes Due To PregnancyDocument21 pagesPhisiological Changes Due To PregnancyVijith.V.kumarNo ratings yet
- OccipitoposteriorDocument11 pagesOccipitoposteriorVijith.V.kumar100% (1)
- Staff Orientation, Training and DevelopmentDocument57 pagesStaff Orientation, Training and DevelopmentVijith.V.kumarNo ratings yet
- Inservice EducationDocument4 pagesInservice EducationVijith.V.kumar50% (2)
- Advance Cardiac SuppDocument32 pagesAdvance Cardiac SuppVijith.V.kumarNo ratings yet
- Antenatal Assessment FormatDocument9 pagesAntenatal Assessment FormatVijith.V.kumar93% (14)
- EngorgementDocument1 pageEngorgementVijith.V.kumarNo ratings yet
- Intranatal Assessment Kempegowda College of Nursing, V.V.Puram, B'Lore-04Document8 pagesIntranatal Assessment Kempegowda College of Nursing, V.V.Puram, B'Lore-04Vijith.V.kumar100% (1)
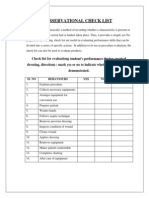
- 30.observational Check ListDocument1 page30.observational Check ListVijith.V.kumarNo ratings yet
- Anecdotal RecordDocument13 pagesAnecdotal RecordVijith.V.kumar100% (1)
- Dhana's FinalDocument73 pagesDhana's FinalNurul magfirahNo ratings yet
- ICD-10 2006 Alphabetical Index (Volume 3)Document770 pagesICD-10 2006 Alphabetical Index (Volume 3)api-3835927100% (3)
- Ob10 Abnormal LabourDocument76 pagesOb10 Abnormal LabourFazzril HasmiNo ratings yet
- OngmcqsDocument26 pagesOngmcqsMoody Summour67% (3)
- Surat Penugasan KlinisDocument13 pagesSurat Penugasan KlinisSischa Afriyani PasaribuNo ratings yet
- OB - Leopold's ManeuverDocument2 pagesOB - Leopold's ManeuverRalph Alfonse De Jesus50% (2)
- Uterine CancerDocument20 pagesUterine Cancerzyrine jhen100% (4)
- Common Surgical Procedure1Document4 pagesCommon Surgical Procedure1Sheana TmplNo ratings yet
- MODULE 1-Lesson 1Document17 pagesMODULE 1-Lesson 1JOHN BRAINARD PEJONo ratings yet
- Obstetric Abdominal Examination OSCE GuideDocument16 pagesObstetric Abdominal Examination OSCE GuideMuhammad Aamir IqbalNo ratings yet
- Answer: Chapter 1 Introduction To Scientific InvestigationDocument13 pagesAnswer: Chapter 1 Introduction To Scientific InvestigationhidayahNo ratings yet
- Procedure Guide Leopold's ManeuverDocument3 pagesProcedure Guide Leopold's ManeuverAubrey Justine GaleonNo ratings yet
- Prospectus New India Floater Mediclaim 21012020 - 1Document20 pagesProspectus New India Floater Mediclaim 21012020 - 1mail2sranjanNo ratings yet
- Ebook Concise Clinical Embryology An Integrated Case Based Approach PDF Full Chapter PDFDocument67 pagesEbook Concise Clinical Embryology An Integrated Case Based Approach PDF Full Chapter PDFdarrel.hoffman255100% (30)
- Caesarian Section: by Bugingo Julita and Abdullahi Muhibba Tutor DR Wanyama JohnDocument46 pagesCaesarian Section: by Bugingo Julita and Abdullahi Muhibba Tutor DR Wanyama JohnBugingo Julita100% (2)
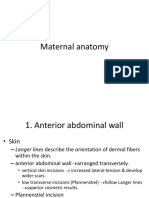
- Maternal AnatomyDocument60 pagesMaternal AnatomyRaraNo ratings yet
- Sessão 2 - Spencer, H - Structure, Function and Evolution, Pp. 67-92Document16 pagesSessão 2 - Spencer, H - Structure, Function and Evolution, Pp. 67-92Palloma MenezesNo ratings yet
- Gas Paper of Obs &obs Nursing PDFDocument18 pagesGas Paper of Obs &obs Nursing PDFyasodha maharajNo ratings yet
- Class: 10 BiologyDocument12 pagesClass: 10 BiologyRehan PervaizNo ratings yet
- Final Exam Review - Bio 172Document21 pagesFinal Exam Review - Bio 172Erin McElhaney QuirkNo ratings yet
- Ectopic PregnancyDocument25 pagesEctopic Pregnancyfred_chandh88No ratings yet
- The Biology of Evil - Part 2Document65 pagesThe Biology of Evil - Part 2Gavin Soccorso100% (1)
- The Female Reproductive SystemDocument7 pagesThe Female Reproductive SystemPavel OnofreiNo ratings yet
- Exam - For MID12.6.10Document4 pagesExam - For MID12.6.10sarahhNo ratings yet
- Block 1 Essay Question and Answers (MBBS)Document188 pagesBlock 1 Essay Question and Answers (MBBS)jdfNo ratings yet
- Genital ProlapseDocument30 pagesGenital ProlapseFarida Nur AiniNo ratings yet
- The Role of Arbudahara Taila Uttarbasti in Tubal Blockage InfertilityDocument4 pagesThe Role of Arbudahara Taila Uttarbasti in Tubal Blockage InfertilityResearch ParkNo ratings yet
- Checklist Sesarea SectionDocument5 pagesChecklist Sesarea SectionBidan RS RoyalNo ratings yet
- PPH Introduction 1Document95 pagesPPH Introduction 1regine maeNo ratings yet
- Case Study-Fibroids in PregnancyDocument10 pagesCase Study-Fibroids in Pregnancysimbarashe tangwadzanaNo ratings yet